Your upper back is not weak. Your nervous system is bracing.
Your brain maintains an internal model of your body called the body schema [4]. That distinction matters. If the rounding is weakness, the answer is strengthening. If it is a prediction your body schema is generating because it has decided rounding is the safest option, the answer is something else entirely. This model is not a picture. It is a prediction engine. It takes sensory input from your joints, your skin, your eyes, your inner ear, and it generates a prediction about where every segment of your spine should be, right now, in this gravitational field.
In kyphosis, that prediction says the thoracic spine should be rounded.
Not because the muscles are weak. Because the nervous system has decided that the rounded position is the safest configuration available.
Kyphosis is the condition I see most often described as “just aging.” It is not aging. It is a bracing pattern your nervous system built to protect a body it cannot clearly feel. And that bracing pattern follows a logic you can learn to read.
We have written about why kyphosis is not a weakness problem. This guide goes deeper. Full mechanism. What drives it. Why common approaches have a ceiling. What actually changes the pattern. And what age does and does not determine.
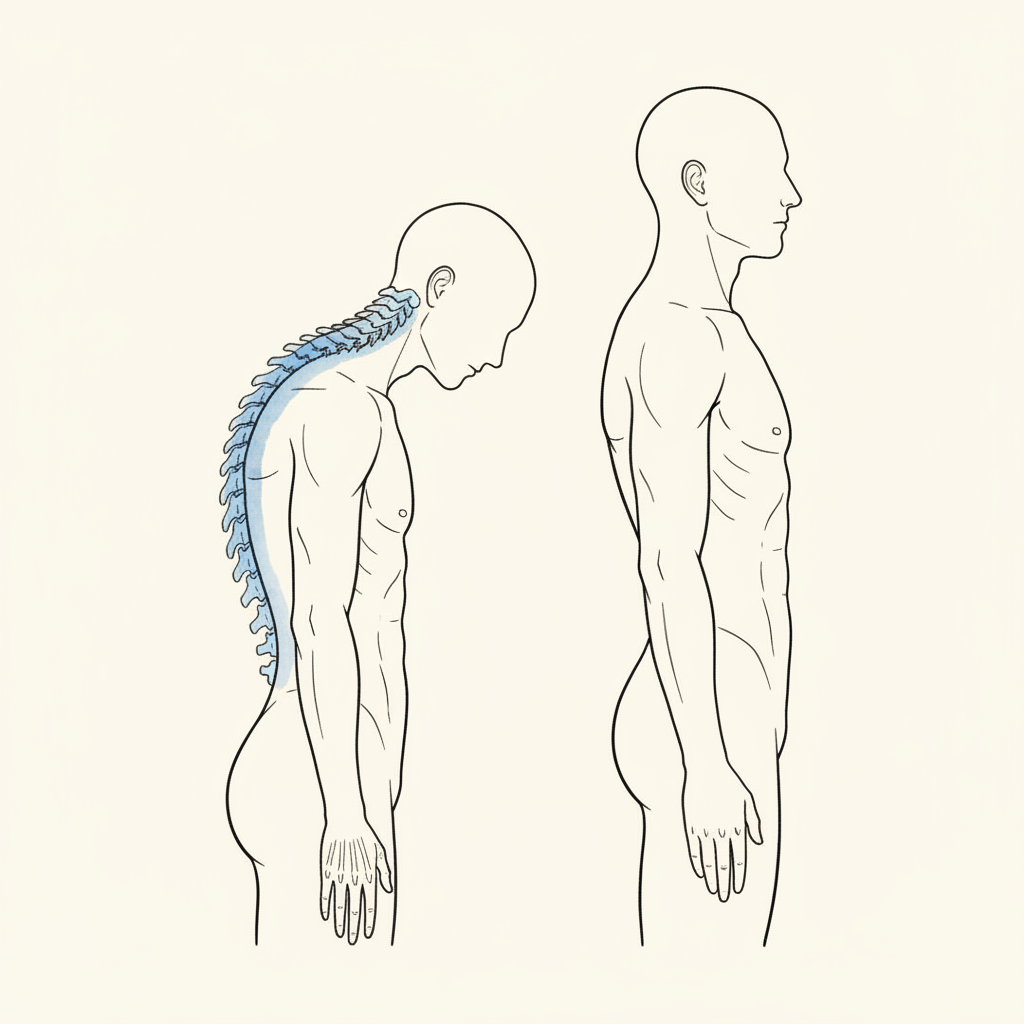
What Kyphosis Actually Is
Kyphosis is an excessive forward curvature of the thoracic spine. Some degree of thoracic curve is normal. Your upper back is supposed to round slightly. The problem begins when that curve deepens beyond what the structure can organize around.
The standard explanation: weak rhomboids, weak lower traps, tight pectorals. Slouching. Poor habits. The fix: rows, band pull-aparts, stretches. Sit up straighter.
The neuroscience explanation is different.
Your brain generates posture as the output of a predictive model [3][5]. That model lives in the parietal cortex [4]. It takes in sensory data. It generates a prediction. The prediction becomes the motor command that organizes your muscles around your skeleton.
Kyphosis is an excessive forward curvature of the thoracic spine. The standard explanation attributes it to weak upper back muscles or poor posture habits. The neuroscience explanation is different. The brain maintains an internal model of the body called the body schema [4]. This model generates predictions about what each segment of the spine should be doing. In kyphosis, the nervous system has generated a prediction that the thoracic spine should be rounded. The rounding is not a collapse. It is an active holding pattern. Research on motor reorganization [8] shows that the brain restructures its motor strategy under conditions of pain, threat, or compromised sensory input. The thoracic rounding is part of a larger pattern called systemic extension, where the nervous system braces the body’s posterior chain because it cannot clearly locate itself in space. The cause is upstream of the muscles between the shoulder blades. It is in the nervous system’s spatial prediction.
Kyphosis is not a weakness in the muscles between your shoulder blades. It is the nervous system’s systemic extension pattern expressed through the thoracic spine. The rounding is protection, not collapse.
Why It Happens: The Nervous System Explanation
Here is where most kyphosis content stops short. It names posture or muscle imbalance as the cause and moves directly to exercises. But the muscles are not making this decision. The brain is.
Three things are happening upstream of the rounding.
The nervous system is in a protective state. When the nervous system detects threat, whether physical pain, chronic stress, or simply degraded sensory input, it organizes the body around protection [1]. This is not a choice. It is a descending signal from the midbrain that reorganizes muscle tone throughout the entire body. The safety hierarchy is sequential: safety first, then sensory processing, then motor output. Under threat, the system never reaches the motor layer where “good posture” lives.
The brain’s map of your upper back has degraded. Research on cortical reorganization [6][7] shows that when a body region is held in a fixed position for long enough, the brain’s sensory map of that region blurs. This is called cortical smudging. The somatosensory cortex loses resolution. You may have reduced ability to feel the space between your shoulder blades with any precision. The brain cannot update a map for a region it cannot feel.
The dominant sensory inputs are driving the head forward. Vision and jaw are the two highest-weighted inputs into the brain’s postural model. They override everything below them. Forward head posture, which invariably accompanies kyphosis, is not a neck pain problem. It is a sensory compensation. The skull moves anterior to bring the focal visual channel into dominance when peripheral vision degrades. The tech neck pattern is a symptom of this hierarchy, not a cause.
These three factors create the rounding. Not weak muscles. Not bad habits. A nervous system that is protecting, a brain map that has degraded, and sensory inputs that are pulling the skull forward. The thoracic spine is caught in the middle.
Systemic Extension: The Full Pattern
Kyphosis does not happen in isolation. It is one expression of a full-body pattern.
When the nervous system cannot clearly locate itself in space, it produces what clinicians call systemic extension. The pattern includes: bodyweight shifts forward, knees hyperextend, the pelvis tilts anterior, lumbar lordosis increases, the chest wall elevates, the shoulders round forward, the head and neck project anterior.
Every item on that list is connected. One pattern.
The chest wall elevation is critical. When the rib cage is held high by the extension pattern, the diaphragm is conscripted into the brace [9]. It cannot organize deep core pressure while it is holding the rib cage elevated. This means the primary anticipatory stabilizer of the spine is offline. The thoracic spine rounds further because it has lost its internal support.
The forward head position is equally critical. The skull moves anterior to compensate for degraded peripheral and ambient vision. The suboccipital muscles at the base of the skull have the highest sensory density of any muscles in the body: 36 spindles per gram [10]. When these muscles are hypertonic from holding the head forward, they are sending a constant stream of tension signals to the brain. This reinforces the protective state.
The kyphosis you see in the mirror is the thoracic spine’s expression of a pattern that starts in the nervous system’s assessment of safety, runs through the sensory hierarchy, and lands in the muscles as a holding pattern.
Treating the thoracic spine without addressing the pattern is like turning off the smoke alarm and calling it fire prevention.
Why Common Treatments Have a Ceiling
If you have kyphosis, you have probably tried some version of the following. Rows and reverse flies. Band pull-aparts. Thoracic extension over a foam roller. Doorway stretches. Dead hangs. Postural reminders.
I hear this constantly. Marcus, a 42-year-old software engineer with kyphosis he has been working on for over a decade, put it this way: “I have been doing dead hangs for two years. I genuinely do not know if they are doing anything.”
He is not wrong to be uncertain. The exercises are real. The muscles exist. They do fire. But three problems prevent them from changing the pattern.
Exercise programs for kyphosis typically target the rhomboids, lower trapezius, and thoracic extensors. These muscles are real and they do work. But the brain is not recruiting them because it has decided that the rounded position is the safest configuration available. This is not laziness or weakness. Research on polyvagal theory [1] shows that the nervous system organizes the body around perceived safety before it organizes around alignment or performance. In the predictive processing framework [3][5], the brain generates motor outputs based on its internal model. Instructing the muscles to contract differently without changing the model produces temporary overrides that revert when conscious effort stops. The instruction “pull your shoulders back” generates a motor command, which produces an efference copy, which cancels the sensory feedback that would update the model. The exercise confirms the brain’s existing prediction rather than challenging it.
Problem one: the brain cannot feel what you are training. If cortical smudging has degraded the brain’s map of your thoracic spine [6], then motor commands to that region arrive at a blurred address. You are sending mail to a house with no number. The muscles may contract, but the brain does not integrate the feedback clearly enough to update its model.
Problem two: the instruction cancels itself. “Pull your shoulders back” is a voluntary motor command. The brain generates it. The brain also generates a prediction of what that movement should feel like. This is called an efference copy. When the expected sensation matches the actual sensation, the brain cancels the signal. No prediction error. No model update. No change. This is why posture keeps going back to where it was.
Problem three: the protective state is still running. The nervous system security system filters sensory input under threat. If the system is still in a protective state, it is suppressing sensory signal from the thoracic region. Stretching a region the brain is actively guarding triggers more guarding, not less. Strengthening a region the brain is protecting does not override the protection. It reinforces the brain’s assessment that the region needs protecting.
Marcus does not need more rows. He needs his nervous system to stop bracing his thoracic spine. And he needs his brain to be able to feel the region it is bracing.
What Actually Changes the Pattern
If kyphosis is a prediction, you need to change the prediction. Not override it. Change it.
The research points to three conditions that must be met for the brain’s body schema to update [3][5][6].
Condition one: sufficient precision. The sensory signal arriving at the brain must be clear enough to register as meaningful. A blurred signal from a smudged region does not update anything. The signal must arrive with enough resolution that the brain treats it as new information.
Condition two: an open gate. The brain’s security system must not be filtering input from the region in question. Under threat, sensory data from the thoracic spine is suppressed before it reaches the cortex. The gate must open. This requires the nervous system state to shift out of protection. Safety is not a warm-up. It is a prerequisite.
Condition three: no efference copy cancellation. The brain must receive sensory information it did not predict. If the sensation matches the brain’s expectation, it is cancelled and produces no update. This is why trying harder to stand straight does not work. The brain predicted the effort. It predicted the sensation. No surprise. No update.
Effective treatment for kyphosis addresses the prediction that generates the rounding, not the rounding itself. Three components appear necessary based on the research. First, the nervous system state must shift. Under threat or chronic stress, the thalamic reticular nucleus suppresses sensory input from the thoracic region, the mechanism behind cortical smudging described by Moseley [6]. The body cannot update a map for a region it cannot feel. Second, the brain’s sensory resolution for the thoracic spine must be restored. Two-point discrimination training and directed attention practices improve the cortical map quality for regions that have become neurologically dark [6]. Third, the brain needs sensory evidence it did not predict. Pandiculation, described by Thomas Hanna [2] as voluntary contraction followed by extremely slow conscious release, gives the brain cortical access to muscles it had lost control over through Sensory Motor Amnesia. The combination addresses the nervous system state, the sensory map, and the motor prediction.
When these three conditions are met, the body schema updates. The prediction changes. The posture changes. Not because you forced it. Because the model that generates it received new information.
This is the sequence that matters. Shift the nervous system state. Restore the sensory map. Deliver evidence the brain did not predict. In that order.
Thomas Hanna [2] identified this decades ago. He called the thoracic holding pattern Sensory Motor Amnesia: the brain’s loss of voluntary control over chronically held muscles. The brain forgets how to release what it has been gripping. His approach, pandiculation, involves voluntarily contracting the muscles that are already holding, then releasing them with extreme slowness. The voluntary engagement gives the brain cortical access to the pattern. The slow release gives the brain a sensory signal it did not predict. The combination restores control.
This is not stretching. Stretching applies force to a muscle the brain is protecting. Pandiculation gives the brain access to a muscle it has lost control over. Different mechanism. Different result.
The diaphragm must also come back online [9]. If the chest wall is held high by the extension pattern, the diaphragm cannot descend to create deep core pressure. Restoring diaphragmatic function is not a breathing exercise in the conventional sense. It is returning the body’s primary anticipatory stabilizer to its stabilizing role.
And the sensory inputs at the top of the hierarchy, vision and jaw, must be addressed. If peripheral vision is degraded and the skull is migrating forward to compensate, no amount of thoracic work will hold because the input driving the forward head is still running.
Kyphosis and Age: What Changes and What Does Not
Ray is 61. Retired engineer. His thoracic kyphosis has been deepening for a decade. His grandkids ask him why he is bent over.
That question is painful. And the conventional answer makes it worse. Because the conventional answer is: this is what happens when you age. The spine degenerates. The discs thin. The curve deepens. Manage it. Accept it.
Here is what the research actually says.
Kyphosis can change in adults, but the mechanism is not what most people expect. Strengthening the upper back muscles does not reverse kyphosis because kyphosis is not caused by weak muscles. The brain is actively holding the thoracic spine in its rounded position. Cortical smudging research [6] shows that the brain’s sensory map of the thoracic region degrades under chronic postural patterns. The person may have reduced ability to even feel their upper back accurately. Exercises targeting muscles the brain cannot properly sense produce limited and temporary results. The brain’s body schema generates the postural prediction from the parietal cortex [4], and correcting the output at the muscular level without updating the prediction at the neural level produces change that reverts. Lasting change requires restoring the brain’s sensory resolution for the thoracic spine, shifting the nervous system out of its protective bracing state, and providing new sensory evidence that the brain did not predict. The timeline varies by severity and duration.
Age is real. The accumulated time under the pattern increases the brain’s confidence in its prediction. In the predictive coding framework [3], longer-held patterns develop higher precision priors. The brain trusts its old prediction more. This means updating the model takes more time and more repetition.
But the mechanism is the same at 61 as it is at 42. The nervous system still responds to safety signals. The cortical map still updates when given clear sensory input. Pandiculation still restores cortical access to muscles held in Sensory Motor Amnesia [2].
What age does: slows the timeline. Increases the repetitions needed. Requires more patience with the sensory restoration phase.
What age does not do: make the mechanism unavailable. The brain remains plastic. The body schema remains updatable. The nervous system remains responsive to conditions of safety.
Ray’s kyphosis is not aging. It is a prediction his nervous system has been reinforcing for decades. The prediction is strong. But it is still a prediction. And predictions update when the conditions are right.
Why Kyphosis Gets Worse (and How to Interrupt the Cycle)
Kyphosis worsens not because the spine is degenerating but because the prediction is consolidating.
The logic is circular. The brain generates the rounded posture as a protective prediction. That posture changes the sensory input the brain receives. Forward head position shifts vision toward focal dominance. The diaphragm stays locked high [9]. The thoracic spine’s cortical representation degrades further [6][7]. The new, degraded input confirms the prediction and strengthens it.
Kyphosis tends to worsen because the nervous system’s prediction model is self-reinforcing. The brain generates the rounded posture as a protective prediction. That posture changes the sensory input the brain receives: forward head position shifts vision toward focal dominance, the diaphragm is locked high by the elevated chest wall [9], and the thoracic spine’s cortical representation degrades further [6]. The new, degraded input confirms the prediction and strengthens it. This is what predictive coding researchers call a self-fulfilling prophecy at the neural level: the prediction generates the posture, the posture generates the sensory input, the sensory input confirms the prediction. Each cycle deepens the pattern. Age is a factor because accumulated time under the pattern increases the brain’s confidence in its prediction, creating higher precision priors [3]. The mechanism is the same at any age. The pattern worsens not because the spine is degenerating but because the prediction is consolidating. Interventions that interrupt the cycle can reverse the consolidation.
This is why doing nothing is not neutral. The cycle runs on its own. Each day under the pattern, the prediction deepens slightly. The brain’s map degrades a fraction further.
But the cycle can be interrupted at any point. Change the nervous system state and the gate opens. Restore the sensory map and the brain has new data. Deliver an unpredicted signal and the model updates.
The interruption does not have to be dramatic. It has to be precise. The right sensory input, at the right resolution, under the right nervous system conditions. Consistently.
This is the difference between managing kyphosis and changing it. Management mitigates symptoms. Change interrupts the cycle at the prediction level and gives the brain a reason to generate a different output.
Frequently Asked Questions
Can kyphosis be fully reversed?
It depends on what has happened at the structural level. If the kyphosis is primarily a nervous system holding pattern, meaning the bones and discs are intact but the brain is organizing the spine into a rounded position, then the pattern can change substantially. If there is structural change at the vertebral level (wedging, compression fractures, significant disc degeneration), the structural component sets a floor. But even with structural involvement, the nervous system component is almost always present on top. Changing the nervous system pattern typically produces more change than people expect, because most of what they experience as “structural” is actually the brain’s prediction being maintained by the mechanisms described above.
How long does it take to see change?
Three factors determine the timeline: how long the pattern has been established, how degraded the brain’s sensory map has become, and how much the nervous system is running a protective state. Someone with a 5-year pattern may see meaningful change in weeks. Someone with a 20-year pattern and significant cortical smudging may need months of consistent sensory restoration before the model begins updating. The key variable is not effort. It is whether the conditions for schema updating are being met. Many people work hard at the wrong thing for years. Then they shift to work that meets the three conditions and see change quickly.
Is kyphosis the same as scoliosis?
They are different structural expressions of related upstream mechanisms. Scoliosis is a lateral and rotational deviation. Kyphosis is a sagittal plane deepening. But both are generated by the same body schema prediction system, both involve cortical smudging of the affected region, and both are maintained by the nervous system’s protective organization. The treatment principles overlap: shift the nervous system state, restore the sensory map, deliver evidence the brain did not predict. The specific regions differ. The logic is the same. Someone can have both simultaneously, and frequently does.
—
Written by Sam Miller, founder of Posture Dojo. Sam had an 85-degree kyphoscoliosis diagnosis at 13, was told nothing could be done, and spent the next eight years proving that wrong without surgery. He now teaches the nervous system approach to posture through the Syntropic Core method.
Ready to address the prediction, not just the posture? Learn about Syntropic Core Reset at syntropiccore.com.
Syntropic Core Reset
Most posture programs give you exercises. This one updates the system that generates your posture. Four weeks live with Sam Miller. You learn how the hidden map works, why everything else missed it, and how to give your nervous system the evidence it needs to generate a different pattern. Breath. Ground contact. Safety. Sensory input. Floor to standing. You leave with a daily practice that holds because the map itself has changed.
Limited spots. Next cohort enrolling now.
Sources
- Porges, S.W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation. W.W. Norton.
- Hanna, T. (1988). Somatics: Reawakening the Mind’s Control of Movement, Flexibility, and Health. Da Capo Press.
- Friston, K. (2010). The free-energy principle: a unified brain theory? Nature Reviews Neuroscience, 11(2), 127-138.
- Paillard, J. (1999). Body schema and body image: A double dissociation in deafferented patients. In G.N. Gantchev et al. (Eds.), Motor Control, Today and Tomorrow.
- Clark, A. (2015). Surfing Uncertainty: Prediction, Action, and the Embodied Mind. Oxford University Press.
- Moseley, G.L., & Flor, H. (2012). Targeting cortical representations in the treatment of chronic pain. Neurorehabilitation and Neural Repair, 26(6), 646-652.
- Flor, H., et al. (2003). Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature, 375, 482-484.
- Hodges, P.W., & Moseley, G.L. (2003). Pain and motor control of the lumbopelvic region: effect and possible mechanisms. Journal of Electromyography and Kinesiology, 13(4), 361-370.
- Kolar, P., et al. (2012). Clinical rehabilitation of stabilizing function of the diaphragm. In Rehabilitation of the Spine. Lippincott Williams & Wilkins.
- Schleip, R. (2003). Fascial plasticity: a new neurobiological explanation. Journal of Bodywork and Movement Therapies, 7(1), 11-19.
Comments
3 responses to “Kyphosis: The Complete Guide to Why Your Upper Back Rounds and What Actually Changes It”
[…] The Complete Guide to Kyphosis | Can Scoliosis Exercises Reduce Your Curve? | Why Posture Corrections Don’t […]
[…] The Complete Guide to Kyphosis | Your Diagnosis Described a Shape, Not a Cause | Why Letting Go of Your Posture Feels Dangerous | […]
[…] The Complete Guide to Kyphosis | The TMJ-Posture Connection | Tech Neck Is an Eye Problem | The Kyphosis-Tinnitus […]