Cervical kyphosis. Military neck. Flat neck. Straight neck. Loss of lordosis. Five names for the same thing: your neck lost its curve.
The neck did not make a mistake. Something downstream changed first. The neck followed.
You cannot treat a cervical spine that is compensating for a thoracic spine that is compensating for an autonomic state. That is treating a symptom of a symptom of a symptom.
The Short Answer
Military neck, cervical kyphosis, flat neck, straight neck, and loss of lordosis are five names for one thing: the neck has lost its normal forward curve. It is rarely a problem the neck created. The neck flattens to compensate for something downstream, most often the thoracic spine, the visual system, the jaw, or an autonomic state stuck in threat. That is why chin tucks rarely hold. The curve returns when the system no longer needs to flatten it: calm the autonomic state first, then recalibrate the vision and jaw inputs that set cervical tone.
The neck serves the eyes
Your body schema organizes the cervical spine around one non-negotiable constraint: horizontal gaze [5]. Your eyes must stay level with the horizon. Everything else is secondary.
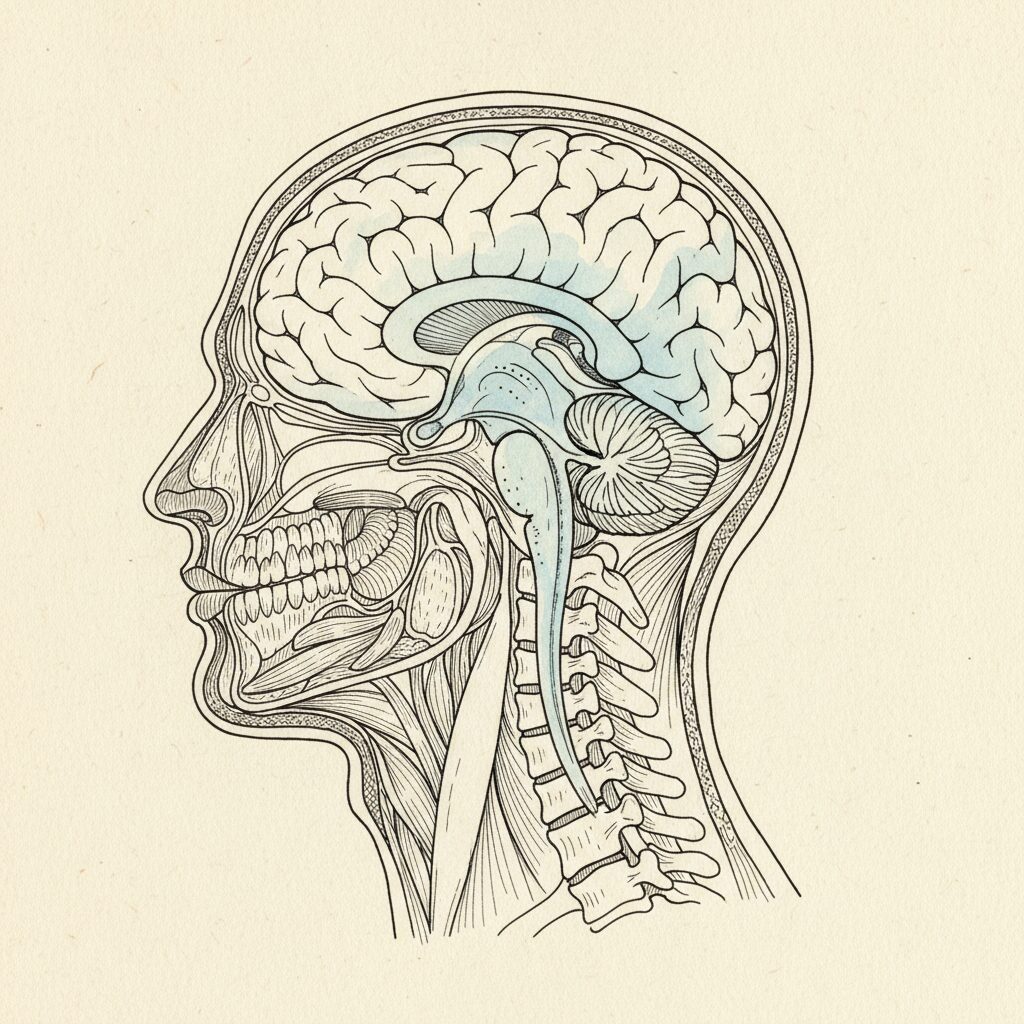
If your thoracic kyphosis increases, your upper body pitches forward. Your eyes would point at the ground. The body schema will not allow that. So it flattens the cervical curve, or reverses it entirely, to bring the eyes back to horizontal.
The cervical kyphosis is not a neck problem. It is a gaze-stabilization solution. The neck lost its curve because the thorax changed, and the system had to compensate to maintain visual orientation.
Harrison [1] modeled this sagittal coupling mathematically. Cervical lordosis is not independent of thoracic kyphosis. They are coupled variables in a single predictive equation. Change one, the other must adjust. The neck is downstream of the thorax in the postural prediction.
Harrison et al. (2005) established the mathematical coupling between thoracic kyphosis and cervical lordosis in sagittal spine modeling. As thoracic kyphosis increases, the cervical spine must flatten or reverse its curve to maintain horizontal gaze orientation. Bruijn et al. (2015) demonstrated that gaze stabilization is a primary constraint on postural organization, with the visual system exerting top-down control over spinal configuration. Kolar (2014) described this within DNS as part of the integrated spinal stabilization system, where cervical position is an output of whole-body postural organization, not an independent variable. The cervical curve is not determined locally. It is computed as the residual adjustment required after thoracic position, pelvic orientation, and visual demands have been satisfied. Treating cervical kyphosis as a neck problem misidentifies an output as a cause.
The two inputs no one checks
Vision and jaw. The two dominant inputs to cervical organization. Almost never assessed in cervical spine treatment.
Your visual system does not just see. It drives postural tone. Ambient vision, the peripheral field, sets the body’s orientation in space. When ambient visual processing is disrupted, the cervical spine compensates. Forward head posture is often a visual compensation, not a muscular weakness.
Your jaw shares a developmental origin with the cervical spine. The trigeminal nerve, which innervates the jaw, converges with cervical afferents in the brainstem. Jaw tension does not stay in the jaw. It feeds directly into the cervical prediction. Hruska [3] mapped this through the PRI Cervical Revolution framework: you cannot resolve cervical position without addressing the jaw’s contribution to the cranial-cervical prediction.
Most cervical kyphosis treatment stretches neck muscles and prescribes chin tucks. It never asks: what are the eyes doing. What is the jaw doing. What is the thorax doing. The neck is the last variable in the equation, and they are treating it first.
The social engagement connection
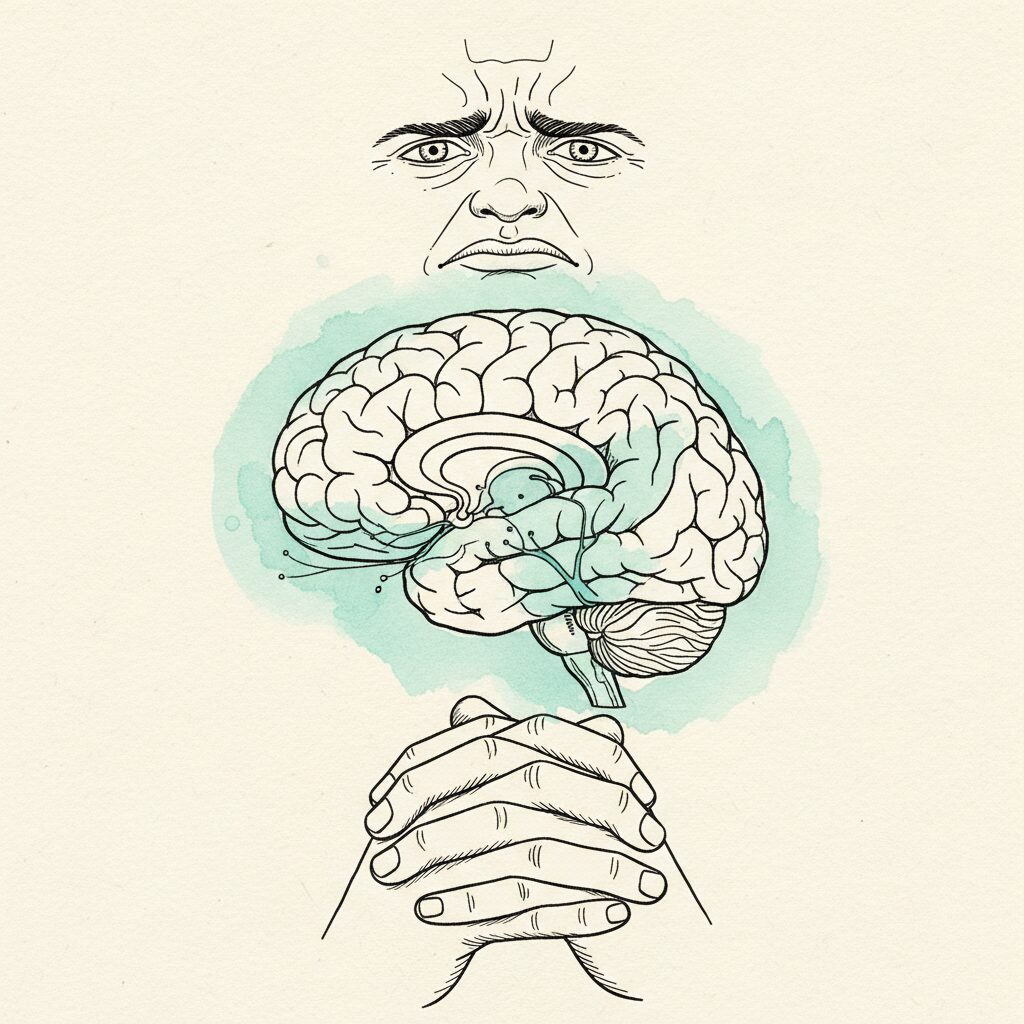
Porges [4] identified something most spine specialists never consider. The social engagement system operates through structures in the head and neck. Cranial nerves V, VII, IX, X, and XI. Facial expression. Vocalization. Listening. Head turning. All of it lives in the cervical region.
When the social engagement system is offline, when the nervous system is in a defensive state, the muscles of the head and neck shift from social signaling to protective bracing. The sternocleidomastoid tightens. The scalenes brace. The suboccipitals lock. The jaw clenches.
Cervical kyphosis is not just a spinal problem. It is a social engagement problem. The neck is flat because the nervous system is not in a state that supports the open, mobile cervical posture required for social engagement.
Porges (2011) established that the social engagement system operates through cranial nerves innervating structures of the head and neck, including muscles of facial expression, middle ear, larynx, pharynx, and head rotation. When autonomic state shifts from ventral vagal (safe, social) to sympathetic or dorsal vagal (defensive), these structures shift from social signaling to protective bracing. The sternocleidomastoid, scalenes, and suboccipital muscles transition from dynamic mobility to tonic contraction. Kolar (2014) described the integrated spinal stabilization system as responsive to autonomic state, with cervical stabilization strategy changing based on the system’s threat assessment. Hruska (2017) mapped the convergence of trigeminal (jaw), visual, and cervical inputs in the PRI Cervical Revolution framework, demonstrating that cervical position cannot be resolved without addressing the dominant sensory inputs that drive cervical tone. The flat neck is not a structural failure. It is the cervical signature of a defensive autonomic state.
Why neck exercises do not work
Chin tucks strengthen the deep cervical flexors. They do not change the thoracic prediction that flattened the cervical curve. They do not address the visual input that is driving forward head position. They do not resolve the jaw tension that is feeding into cervical tone. They do not shift the autonomic state that took the social engagement system offline.
The neck will find its curve when the system no longer needs to flatten it.
That requires working in order. Autonomic regulation first, because cervical tone is downstream of autonomic state. Sensory recalibration second, addressing the dominant inputs: vision, jaw, vestibular. Organized internal pressure third, updating the thoracic prediction that the cervical spine is compensating for.
The neck is last. Not because it does not matter. Because it cannot change until everything upstream has changed first.
—
Related: The Complete Guide to Kyphosis | The TMJ-Posture Connection | Tech Neck Is an Eye Problem | The Kyphosis-Tinnitus Connection
—
Syntropic Core Reset addresses the whole-spine prediction. It starts with autonomic regulation, which affects cervical tone through the social engagement system. Then sensory recalibration of the dominant inputs: vision, jaw, vestibular. Then organized internal pressure updating the thoracic prediction. The neck finds its curve because the system no longer needs to flatten to maintain gaze. See the full approach.
Frequently Asked Questions
What is military neck?
Military neck (also called cervical kyphosis or flat neck) is when the neck loses its normal forward curve. It signals the neck is compensating for something downstream, not a problem the neck created.
What causes military neck?
The cervical spine flattens to compensate for an upstream driver: a thoracic prediction, disrupted ambient vision, jaw tension, or an autonomic state in threat. The neck follows; it does not lead.
Can military neck be corrected?
Often, but not by forcing the curve back. The neck regains its curve when the system no longer needs to flatten it: regulate the autonomic state and recalibrate vision and jaw, in that order.
Why do not chin tucks fix military neck?
Chin tucks strengthen the deep cervical flexors but do not change the thoracic prediction, the visual input, the jaw tension, or the autonomic state driving the flattening. They address the output, not the cause, so the curve returns.
Sources
- Harrison, D.E., Harrison, D.D., Janik, T.J., et al. (2005). Modeling of the sagittal cervical spine as a method to discriminate hypolordosis. Spine, 29(22), 2485-2492. PMID: 15543059 [T1]
Established mathematical coupling between thoracic kyphosis and cervical lordosis. Cervical curve is not an independent variable. It is computed as a function of thoracic position and gaze-stabilization requirements. - Kolar, P. (2014). Clinical Rehabilitation. Alena Kobesova, ed. Prague: Rehabilitation Prague School. [T1]
Describes the integrated spinal stabilization system where cervical position is an output of whole-body postural organization. Cervical stabilization strategy changes based on autonomic state and developmental motor patterns. - Hruska, R. (2017). PRI Cervical Revolution. Postural Restoration Institute. [T2]
Maps the convergence of trigeminal, visual, and cervical inputs driving cervical position. Demonstrates that cervical spine treatment without addressing jaw and visual contributions treats the compensation, not the cause. - Porges, S.W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-regulation. W.W. Norton. [T1]
The social engagement system operates through head and neck structures. When autonomic state shifts to defense, cervical muscles shift from social signaling to protective bracing. Cervical kyphosis is a social engagement problem, not just a spinal one. - Bruijn, S.M., van Dieen, J.H., Meijer, O.G., & Beek, P.J. (2015). Is slow walking more stable? Journal of Biomechanics, 42(10), 1506-1512. [T1]
Demonstrated gaze stabilization as a primary constraint on postural organization. The visual system exerts top-down control over spinal configuration, making cervical position subordinate to gaze-horizon requirements.
Related research
- Best Exercises for Kyphosis: What Actually Changes the Curve
- Your Kyphosis Is Not a Mistake Your Body Made
- Kyphosis and Ankylosing Spondylitis: What Surgery Can and Can’t Change
- That Numb Spot in Your Upper Back Isn’t Dead Tissue