Your upper traps will not soften. Your hip flexors retighten overnight. Your jaw clenches while you sleep, and you wake up with the same knot between your shoulder blades that was there yesterday and the day before that and the day before that.
You have stretched them. You have rolled them. You have paid someone to dig their elbow into them. And every time, the relief lasts a few hours before the tightness rebuilds itself in the exact same pattern.
This is not a muscle problem. This is not a flexibility problem. This is a pressure problem. And until you understand that, the cycle will not break.
Your tight muscles are not broken. They are working.
Every tight muscle in your body is solving a problem. Not the problem you think. Not “I am inflexible” or “I carry stress in my shoulders.” A structural problem. A stability problem. A problem your conscious mind does not even know exists.
Your body runs two stabilization systems. The first is hydraulic. It uses internal pressure, generated by the diaphragm, pelvic floor, and deep abdominal wall, to support the spine from the inside out. This system is automatic, anticipatory, and energy-efficient. It fires before you need it, adjusts continuously, and costs almost nothing to maintain [1].
The second is muscular tension. It uses superficial muscles, your traps, your erectors, your hip flexors, your jaw, to grip the skeleton into position from the outside. This system is reactive, conscious, and energy-expensive. It is your body’s backup generator.
Most people have been running on the backup for years.
Hodges and Richardson (1999) demonstrated that patients with low back pain show delayed activation of deep stabilizers (transversus abdominis, multifidus) and compensatory overactivation of superficial global muscles. The deep stabilization system, which generates intra-abdominal pressure for hydraulic spinal support, fails to fire anticipatorily. In its absence, the nervous system recruits superficial muscles to provide the stability the pressure system is no longer generating. This is not a muscle tightness problem. It is a stabilization strategy substitution: tension replacing pressure.
A map of what your tension is compensating
The tension is not random. The nervous system chose these specific muscles for specific structural reasons.
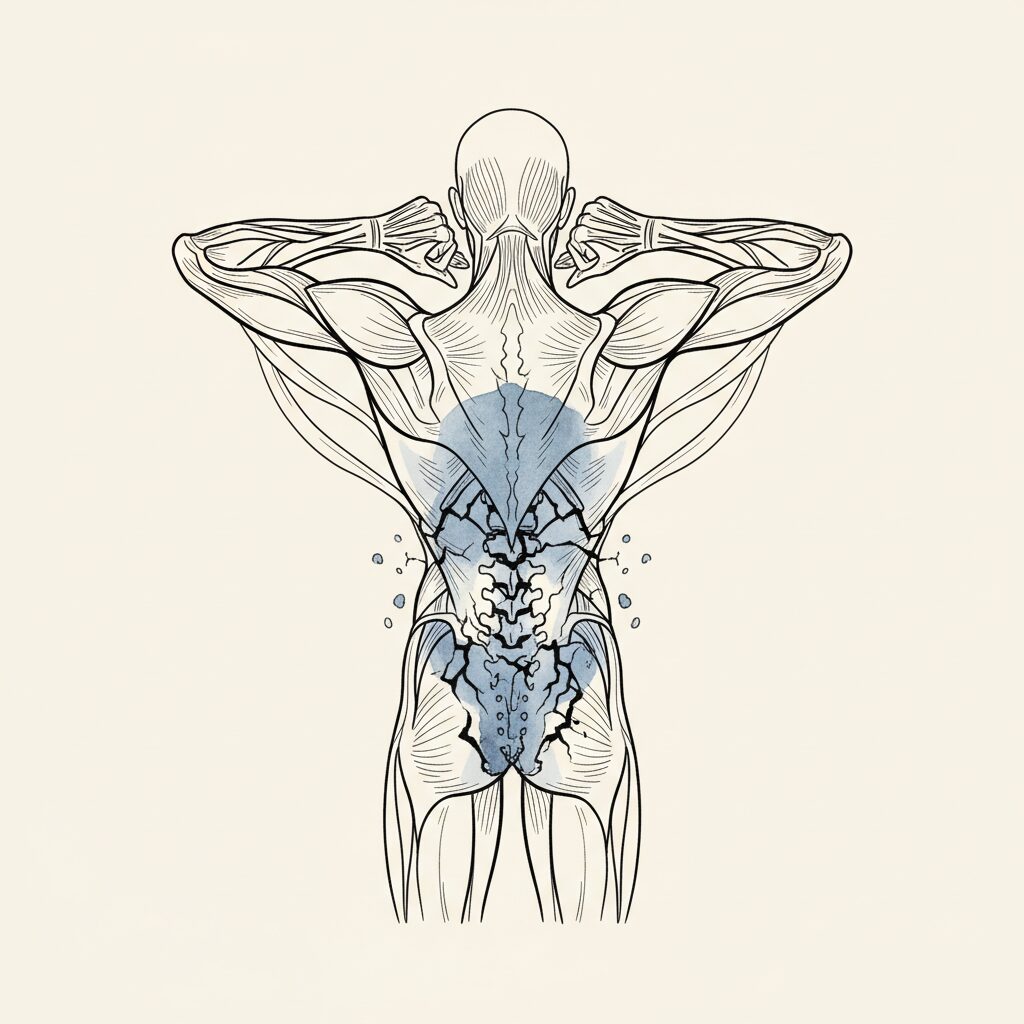
Tight upper traps. Your traps are gripping to provide vertical support that your intra-abdominal pressure is no longer generating. When the pressure canister loses its upward force vector, the traps take over from above. They are literally holding your head and shoulders up because the hydraulic lift from below has dropped.
Gripping hip flexors. Your psoas and iliacus are bracing the front of the pressure canister. When the anterior wall of the pressure system, the transversus abdominis, stops generating adequate tension, the hip flexors stiffen to prevent the pelvis from losing its position. They are doing the job the deep abdominal wall abandoned.
Locked jaw. Your masseter and temporalis are bracing the top of the pressure column. The jaw sits at the superior end of the fascial chain that runs from the pelvic floor to the cranium. When pressure is not being generated at the bottom, the top compensates by locking down. The jaw is not tense because you are stressed. The jaw is tense because the floor of the pressure system is not doing its job.
Thoracolumbar grip. The erector spinae along your mid and lower back are splinting the spine that is no longer receiving hydraulic support. Hodges showed that IAP alone provides 8 to 31 percent of spinal stiffness [1]. When that pressure drops, the erectors take over. They brace the spine from behind because nothing is supporting it from within.
Why releasing the tension does not work
Now you can see why stretching provides temporary relief. You are lengthening a muscle that is under active orders to stay short. The stretch temporarily overrides the command. The nervous system pauses the compensation. For a moment, you feel looser.
Then the nervous system surveys the situation. The pressure system is still offline. The spine still needs stabilization. The demand has not changed. The order goes back out. The muscle retightens. Not because the stretch failed. Because the compensation is still needed.
Massage works the same way. The therapist releases the grip. The nervous system rebuilds it within hours. The compensation is load-bearing. Remove it without replacing it and the system re-tensions because it has no other option.
Moseley and Hodges showed this directly: even after pain resolves completely, the tension strategy persists [4]. The pain is gone. The rigidity remains. Because the system never returned to the pressure-based strategy. It has been running on the backup so long that the backup became the default.
Moseley and Hodges (2006) demonstrated that motor strategy changes induced by back pain persist even after pain resolution. The reduced variability of postural strategy, characterized by increased superficial muscle guarding and decreased deep stabilizer activation, becomes self-sustaining. Kolar et al. (2012) showed the mechanism: flattened diaphragm position reduces pressure generation capacity, maintaining the conditions that require compensatory tension. The tension pattern is not a residue of pain. It is an active stabilization strategy responding to an ongoing pressure deficit. Releasing the tension through stretching or manual therapy addresses the compensation without restoring the system it compensates for, explaining the universal clinical observation that chronic tightness returns within hours of treatment.
The muscle your body actually needs
The transversus abdominis is the only trunk muscle that varies its activation with vertical center-of-mass position regardless of load direction [5]. It does not care which way you are being pushed. It responds to gravity itself. It is not a movement muscle. It is a pressure muscle. When it fires, the pressure canister pressurizes. When it does not fire, the backup generators take over.
You cannot strengthen the transversus into doing its job by doing planks or crunches. Those exercises use the rectus abdominis and the obliques, the tension system. They build more backup capacity. They do not restore the primary.
The transversus, the diaphragm, the pelvic floor, the multifidus. These are pressure muscles. They generate the hydraulic support that makes the tension muscles unnecessary. And they do not respond to instructions. They respond to conditions.
The faster way
Syntropic Core Resets do not target tight muscles. They do not stretch what grips. They do not try to release the compensation.
They restore the pressure system underneath.
When the diaphragm recovers its dome. When the deep stabilizers begin firing anticipatorily again. When intra-abdominal pressure returns to its automatic, gravity-responsive function. The nervous system does something remarkable. It decommissions the compensations it no longer needs.
The traps soften. The hip flexors release. The jaw unlocks. Not because you targeted them. Not because you stretched them. Because the system they were compensating for came back online. Their job ended. They stood down.
This is why people report tension releasing in muscles they did not even work on during a reset. Because the pressure system does not operate muscle by muscle. It operates as a whole. When the primary comes back, the backup shuts off everywhere at once.
You are not too tight. You are under-pressurized. And the path out is not more releasing. It is restoring the system that makes releasing unnecessary.
—
Related: Why Your Body Holds Tension (Even When Nothing Is Wrong) | The Collapse That Fixes Your Posture | The Fastest Way to Release Tension
—
Syntropic Core Resets restore the pressure system, not by fighting tight muscles but by reactivating the diaphragm and deep stabilizers that make tension unnecessary. See how it works.
Sources
- Hodges, P.W., Eriksson, A.E., Shirley, D., & Gandevia, S.C. (2005). Intra-abdominal pressure increases stiffness of the lumbar spine. Journal of Biomechanics, 38(9), 1873-1880. PMID: 16023475 [T1]
When IAP drops, the spine loses hydraulic stiffness. Superficial muscles compensate with tension to replace the lost stability. IAP alone provides 8-31% of spinal stiffness without voluntary effort. - Hodges, P.W., & Richardson, C.A. (1999). Altered trunk muscle recruitment in people with low back pain with upper limb movement at different speeds. Archives of Physical Medicine and Rehabilitation, 80(9), 1005-1012. PMID: 10489000 [T1]
LBP patients show delayed deep stabilizer activation and compensatory superficial muscle guarding. The nervous system substitutes tension for pressure when the deep stabilization system fails. - Kolar, P., et al. (2012). Postural function of the diaphragm in persons with and without chronic low back pain. Journal of Orthopaedic & Sports Physical Therapy, 42(4), 352-362. PMID: 22236541 [T1]
Flattened diaphragm position reduces pressure generation capacity. The organ that generates hydraulic spinal support is compromised, forcing compensatory tension patterns. - Moseley, G.L., & Hodges, P.W. (2006). Reduced variability of postural strategy prevents normalization of motor changes induced by back pain. Behavioral Neuroscience, 120(2), 474-476. PMID: 16719711 [T1]
Pain locks the system into rigid tension strategies. Even after pain resolves, the tension pattern persists because the pressure system was never restored. - Eriksson Crommert, A., Ekblom, M.M., & Thorstensson, A. (2011). Activation of transversus abdominis varies with postural demand in standing. Gait & Posture, 33(3), 473-477. PMID: 21269831 [T1]
TrA is the only trunk muscle that co-varies with vertical center-of-mass position regardless of load direction. It responds to gravity, not instructions. When it fails, global tension muscles take over.