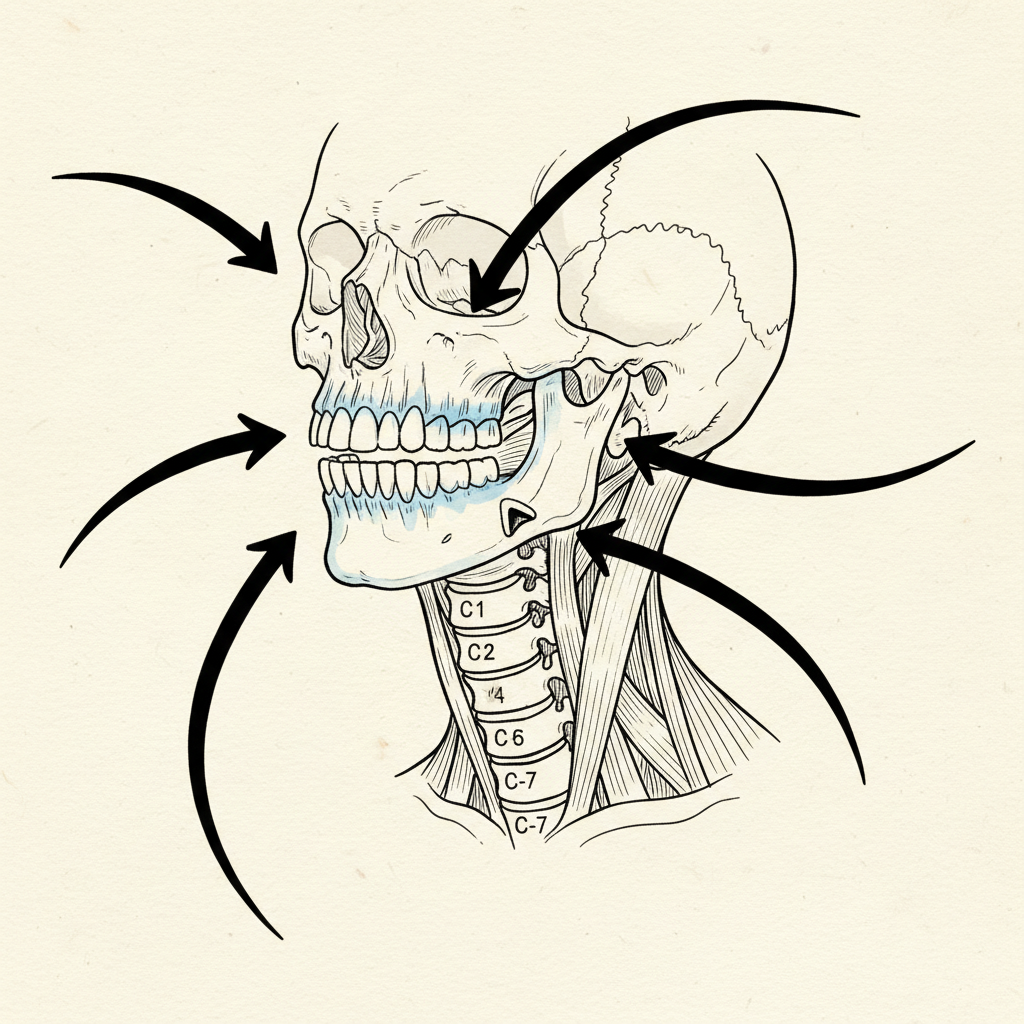
Put your fingers on your jaw joint. Right in front of your ear. Now open your mouth slowly. Feel the condyle move under your fingertips. Feel the click, the hesitation, the asymmetry if it is there.
That is not your jaw talking. That is your whole system.
The jaw and the neck are not neighbors who happen to share a wall. They are wired together at the deepest level of the nervous system’s architecture. Where the jaw goes, the head follows. Where the head goes, the neck compensates. Where the neck compensates, the entire postural chain reorganizes.
The trigeminal nerve outranks your core
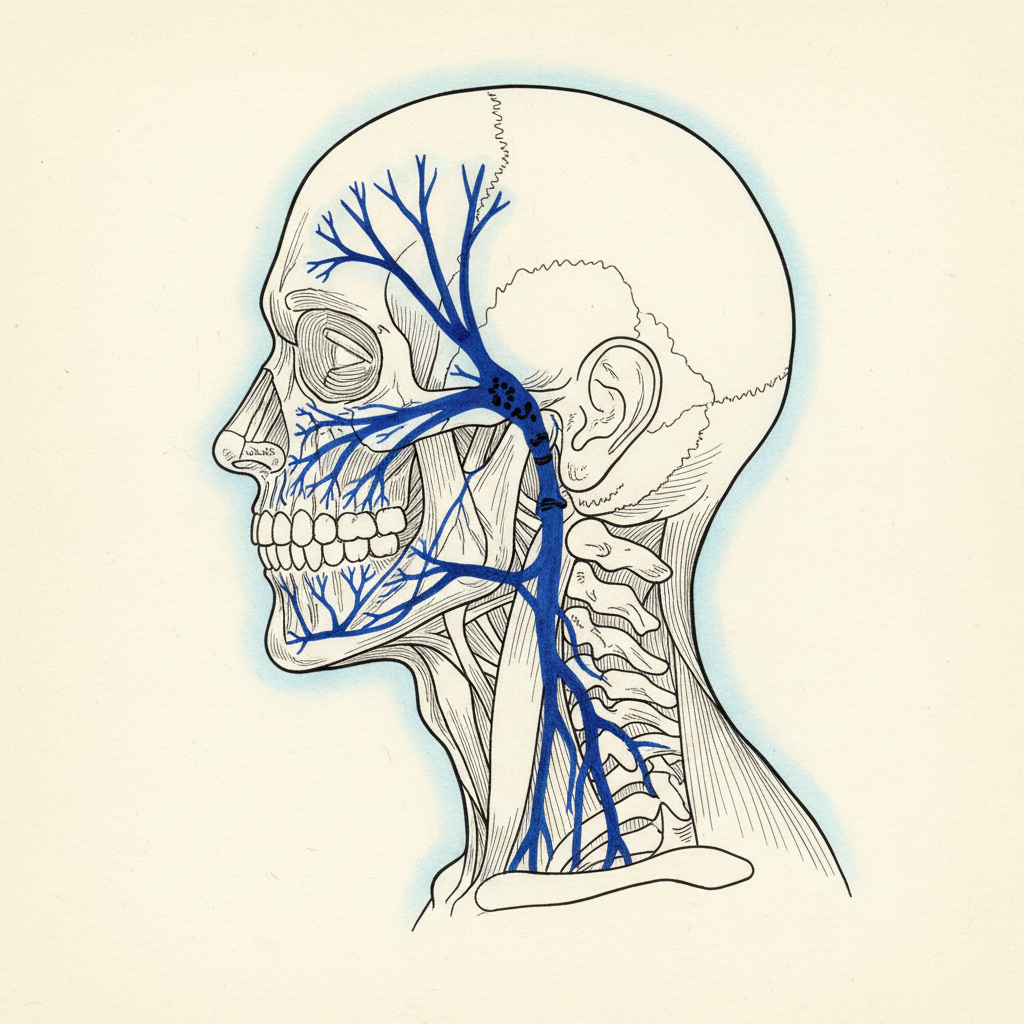
The trigeminal nerve is the fifth cranial nerve. Largest sensory nerve in the head. It innervates the jaw muscles, the teeth, the TMJ capsule, the face, significant portions of the skull. It sends more sensory data to the brainstem than any other cranial nerve.
Here is the detail that changes the picture.
The trigeminal motor nucleus has direct connections to the cervical motor neurons that control neck muscles. Direct. Not routed through higher processing centers. The jaw’s position influences neck muscle tone through a hardwired circuit operating below conscious awareness.
The jaw is not downstream of posture. It is upstream. Jaw dysfunction can drive neck muscle imbalance independently of anything happening in the thoracic spine, the shoulders, or the core. You can do neck exercises for years and see no lasting change if the jaw is corrupting the signal that controls the neck muscles.
In the hierarchy of the body schema’s postural prediction, the jaw is Tier 1. It outranks the core. It outranks the hips. It outranks every input except vision. When the jaw sends corrupted data, the system sacrifices everything below to accommodate what is happening above.
The causation runs both ways
Forward head posture changes jaw biomechanics. When the head sits anterior to the center of gravity, the mandible shifts posteriorly. Condyles reposition. Disc position changes. Muscles of mastication load asymmetrically. Over time: clicking, popping, pain, restriction. TMJ dysfunction.
But jaw dysfunction also drives the head forward. When the bite is asymmetrical, when the teeth do not contact evenly, when the jaw is chronically clenched, the trigeminal nerve signals that the head is not stable relative to the jaw. The system responds by activating the cervical extensors. Suboccipitals fire. SCM compensates. Deep cervical flexors disengage. The head drifts forward because the system is trying to stabilize a skull that has lost its reference point below.
Two outputs of the same input mismatch. The dentist treats one half of the loop. The physical therapist treats the other. The loop itself continues.
Clenching is not a habit
It is a threat response.
The masseter is one of the first muscles to activate under sympathetic arousal. Hardwired survival architecture. Clenching braces the skull against impact. Same reflex that makes you grit your teeth when startled.
In chronic stress, the jaw never fully releases. The masseter maintains low-grade activation around the clock. During sleep, activation intensifies. Bruxism is a sympathetic event. The nervous system runs threat protocols while you sleep, and the jaw is the primary expression.
Follow the chain. Stress activates the jaw. The jaw drives the neck through the trigeminal-cervical circuit. The neck stiffens. The head drifts forward. The thoracic spine rounds. The diaphragm compresses. Internal pressure drops. Reduced pressure lowers vagal tone. Low vagal tone keeps the system in sympathetic dominance. Which activates the jaw.
The loop closes.
Why night guards do not fix this
Night guards protect teeth. They do not address clenching. The masseter still fires. The trigeminal nerve still sends its signal. The cervical compensation still runs.
Same limitation applies to most TMJ treatments. Bite splints reposition the mandible mechanically. Botox reduces masseter force. Jaw exercises increase mobility. Each addresses the jaw as a local system. None addresses its role as a postural input.
Try this right now
Clench your jaw. Hard. Hold it for ten seconds.
Notice what happens in your neck. The suboccipitals fire. The back of the skull tightens. Upper traps engage. Shoulders elevate slightly. Trigeminal-cervical reflex in action.
Now release the clench. Slowly. Let the jaw fall open. Teeth separate. Masseter releases.
Notice the neck. Suboccipitals soften. Traps drop. Head shifts slightly posterior. Not relaxation. Removal of a postural input. The neck was responding to the jaw. When the jaw released, the neck had nothing to respond to.
You just felt the hierarchy.
What actually resolves both together
Sequence matters. You cannot start with jaw exercises if the system is driving clenching through sympathetic activation.
First, reduce the threat state. Extended exhale breathing. Parasympathetic activation through the vagal brake. When the system shifts out of threat mode, the masseter’s baseline activation drops. The system driving the clench received a signal that the threat level has decreased.
Second, restore jaw awareness. Most people with TMJ dysfunction have lost proprioceptive awareness of jaw position. They do not know where their jaw is unless they are actively thinking about it. The body schema’s representation of the jaw has become blurred. Cortical smudging. Gentle, slow jaw movements with full attention begin to restore the sensory resolution the schema needs to work with.
Third, address the bite if it needs addressing. Asymmetrical tooth contact sends asymmetrical trigeminal input with every swallow, every chew, every resting position. That is a hardware issue. Sensory work alone cannot override a structural mismatch. Collaboration with a dentist who understands the postural implications of bite alignment is essential. Not every dentist does.
Fourth, let the chain reorganize downward. Once the jaw input cleans up, the cervical spine responds. Neck muscles that were bracing against corrupted jaw data release. The head repositions. Thoracic spine opens. Diaphragm gets space. Internal pressure returns. The chain reorganizes from the top because the disruption originated at the top.
The hierarchy is not optional
Your TMJ is not separate from your forward head posture. Your forward head is not separate from your neck pain. Your neck pain is not separate from your thoracic kyphosis. One chain, driven from the top by an input that sits inside your mouth.
Laura, a participant with scoliosis and kyphosis who had tried multiple approaches, described what happened when the right inputs were addressed: “With the pressure, it just found the place where it wanted to be.”
The body knows where it belongs. The jaw is either letting it get there or preventing it. Address the jaw, and the chain below has permission to reorganize. Ignore the jaw, and every correction below it is temporary.
Architecture is not negotiable.
Syntropic Core Reset
Most posture programs give you exercises. This one updates the system that generates your posture. Four weeks live with Sam Miller. You learn how the hidden map works, why everything else missed it, and how to give your nervous system the evidence it needs to generate a different pattern. Breath. Ground contact. Safety. Sensory input. Floor to standing. You leave with a daily practice that holds because the map itself has changed.
Limited spots. Next cohort enrolling now.
Details and enrollment →Sources
- Sessle, B.J. (2000). Acute and chronic craniofacial pain: brainstem mechanisms of nociceptive transmission and neuroplasticity, and their clinical correlates. Critical Reviews in Oral Biology & Medicine, 11(1), 57-91. [T1]
Trigeminal nerve as the largest cranial sensory nerve. Direct trigeminal-cervical connections. - Catanzariti, J.F., et al. (2005). Relationship between the jaw and the body posture: literature review. Annales de Readaptation et de Medecine Physique, 48(5), 263-275. [T1]
Jaw position influencing cervical spine posture. Bidirectional relationship between TMJ and forward head. - Porges, S.W. (2011). The Polyvagal Theory. W.W. Norton. [T1]
Jaw clenching as sympathetic threat response. Masseter activation under arousal. - Clark, A. (2015). Surfing Uncertainty: Prediction, Action, and the Embodied Mind. Oxford University Press. [T1]
Jaw as sensory input to the postural prediction. Corrupted jaw data generating compensatory motor output. - Hanna, T. (1988). Somatics: Reawakening the Mind’s Control of Movement, Flexibility, and Health. Da Capo Press. [T1]
Cortical smudging of jaw proprioception. Sensory Motor Amnesia in jaw muscles. - Flor, H., et al. (1997). Extensive reorganization of primary somatosensory cortex in chronic back pain patients. Neuroscience Letters, 224(1), 5-8. [T1]
Cortical smudging concept applied to jaw: loss of proprioceptive resolution in chronic dysfunction. - Lavigne, G.J., Khoury, S., Abe, S., Yamaguchi, T., & Bhatt, P. (2008). Bruxism physiology and pathology: an overview for clinicians. Journal of Oral Rehabilitation, 35(7), 476-494. [T1]
Bruxism as sympathetic event during sleep. Masseter first muscle to activate under arousal.
Related research
- Your Back Pain Is Not Caused by Your Posture (But They Share the Same Source)
- Tech Neck Is Not About Your Phone (It’s About Your Eyes)
- Two Papers Just Landed: The Neural Generation Hypothesis and the Generative Posture Framework
- Stand Up Tall, Pull Your Shoulders Back, Brace Your Core: Why the 3 Most Common Posture Cues Are Neuroscience Dead Ends
Comments
One response to “TMJ and Posture: Why Your Jaw Is Running Your Neck”
[…] The Complete Guide to Kyphosis | The TMJ-Posture Connection | Tech Neck Is an Eye Problem | The Kyphosis-Tinnitus […]