The head that tilts and nobody knows why
She has been tilting her head five degrees to the right since high school. She did not notice it for years. Then she saw a photograph from her wedding and the tilt was so obvious she could not unsee it.
She went to the chiropractor. Cervical adjustment. The tilt came back the next day.
She went to the physical therapist. Strengthening, stretching, postural cues. The tilt came back.
She went to the dentist who said her jaw was off. Splint. The tilt came back.
What nobody asked was whether her inner ear was telling her brain the world was tilted, and her head was simply tilting to make the world look level.
This article is about the sense most patients with chronic posture problems do not know they have. How it works. How it goes wrong. And why so many cases that did not respond to anything else respond when this layer finally gets addressed.
The 148-word answer
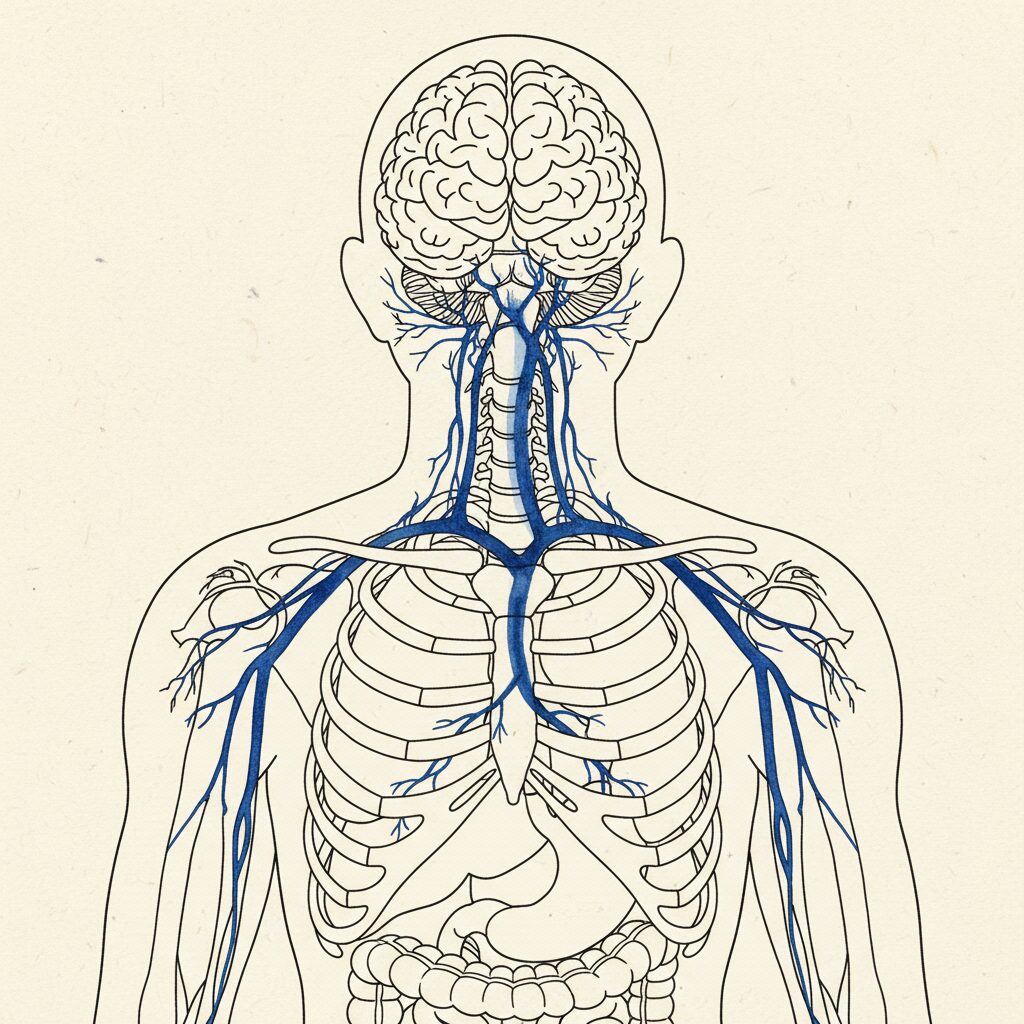
Your inner ear contains a system of fluid-filled canals and tiny crystals that continuously report which way is up, how your head is moving, and whether the world around you is stable. This is the vestibular system. It feeds the postural control circuits in your brainstem alongside vision and proprioception. When the vestibular system is asymmetric (one side weaker, one side over-firing, or the two sides poorly integrated), the brain receives a tilted version of “level” and the body adopts a compensating tilt to make the world appear straight. This shows up as head tilt, shoulder rotation, pelvic shift, and in some cases scoliotic curves. Research has linked vestibular asymmetry to idiopathic scoliosis in both animal models and human studies. Most patients with chronic postural asymmetry never get the vestibular system screened. When it is involved, no amount of structural therapy will hold against an unresolved vestibular driver.
The sense most people don’t know they have
Five classical senses get taught in school. Sight, hearing, smell, taste, touch. Almost nobody is taught about the vestibular system.
The ELI5 version. Inside each of your inner ears is a tiny system of fluid-filled tubes and crystals. Every time you move your head, the fluid sloshes and the crystals tilt, sending signals to your brain about what direction your head is moving and what direction is down. The system is so reliable that you usually do not notice it. You only notice it when something is wrong.
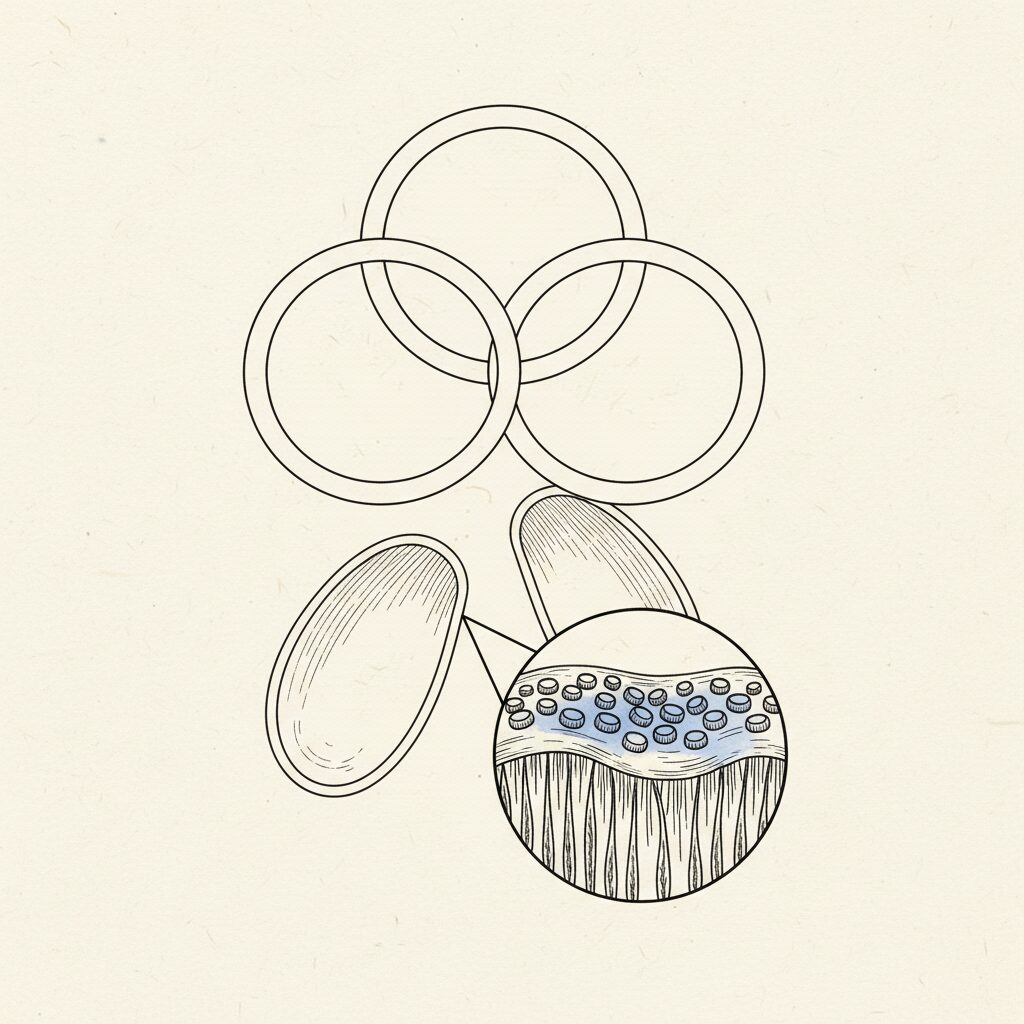
The ELI12 version. The vestibular system has two main parts inside the bony labyrinth of the inner ear. The semicircular canals (three loops oriented at right angles to each other) detect angular acceleration of the head [2]. The otoliths (the saccule and utricle, each containing calcium carbonate crystals on a gelatinous membrane) detect linear acceleration and the direction of gravity. Signals from both feed the vestibular nuclei in the brainstem, which then drive the vestibulo-spinal tracts (controlling postural muscles), the vestibulo-ocular reflex (stabilizing the eyes during head movement), and the cortical pathways that give you a conscious sense of orientation.
In plain language: your inner ear is a continuous spatial GPS. It tells your brain where down is. It tells your eyes how to compensate when your head moves. It tells your spine how tall to stand. Most of this happens below conscious awareness.
How vestibular asymmetry produces postural asymmetry
The brain wants two things from the vestibular system: a stable reading of where down is, and matching information from both sides.
When one side weakens (illness, head injury, infection, age, idiopathic), the brain still receives a signal from that side, but it is quieter than the other. The asymmetry between the two ears tells the brain the head is tilted, even when it is not.
Three things follow.
The eyes compensate. The vestibulo-ocular reflex (VOR) adjusts so the world appears level. This is automatic and unconscious.
The neck compensates. The head tilts physically to one side, putting the inner ear into a position where the asymmetry is reduced. Now the brain receives a reading that feels balanced. From outside, the head looks tilted [3].
The spine compensates. The shoulders and torso rotate to support the new head position. The pelvis shifts to keep the head over the base of support. The entire postural chain reorganizes around an asymmetric input.
Posture is downstream of the brain’s belief about which way is up. If that belief is wrong, no amount of corrective exercise can override it. The system simply restores the posture that makes its inner GPS read correctly.
This is the same logic that makes visual asymmetry produce postural asymmetry. The two systems are tightly coupled. Both feed the brainstem’s orientation circuits. Both have to agree on where level is. When they disagree, the body bends to one of them.
The vestibular link to scoliosis
This is the most under-discussed mechanism in the scoliosis literature, and the evidence is strong enough that it should be a routine part of the workup.
Lambert and colleagues, working at the Paris Descartes vestibular lab, induced scoliotic curves in Xenopus larvae by surgically removing one labyrinth (the vestibular organ on one side) early in development [4]. The animals developed three-dimensional spinal curves with the same morphology as adolescent idiopathic scoliosis in humans. The curves were not random. They were the precise compensation a postural system would make for an asymmetric vestibular input.
Simoneau and colleagues showed in human adolescents with idiopathic scoliosis that the integration of vestibular information with other postural signals is impaired compared to age-matched controls [5]. The vestibular signal was not necessarily weaker on one side, but the brain was not weighting and combining the signals correctly.
The clinical implication is real. Some percentage of adolescent and adult scoliosis cases is being driven, at least in part, by an unresolved vestibular asymmetry. The standard PSSE workup typically does not test for this. The standard pediatric scoliosis assessment does not test for this. The patient is then prescribed Schroth or SEAS or bracing without ever addressing the upstream input that is driving the curve.
Signs the vestibular system may be part of your case
The signs are usually subtle until you know what to look for.
Chronic head tilt that does not respond to neck-specific therapy. The tilt is solving a vestibular asymmetry problem. Correcting the neck does not change the asymmetry.
Motion sickness, especially started or worsened in adulthood. The vestibular system is sending signals that conflict with the visual signal. The conflict produces nausea.
Difficulty in busy visual environments. Grocery store aisles. Open-plan offices. The visual signal is moving but the body is not. Your vestibular system has to filter the conflict, and a compromised system filters poorly.
Dizziness or unsteadiness in the dark or with eyes closed. Without vision to compensate, the underlying vestibular asymmetry becomes detectable.
A history of childhood ear infections, vertigo episodes, or a head injury. Each one can produce lasting vestibular changes.
Difficulty with sports that require head movement. Skiing. Cycling. Yoga inversions. The vestibular system has to recalibrate fast for these activities. A compromised system cannot keep up.
Scoliosis or chronic head/neck postural pattern that plateaued on structural therapy. Plateau is the signal that an upstream input is overriding the corrective work. Vision and vestibular are the most common candidates.
The vestibular workup
A proper vestibular assessment is not what your GP does in the office when they look in your ears.
The workup typically includes videonystagmography (VNG, which tracks eye movements during head positions and caloric stimulation), vestibular evoked myogenic potentials (VEMPs, which test the saccule and utricle directly), and posturography (which measures postural sway under different sensory conditions). Some clinics use the subjective visual vertical test, where the patient adjusts a line to what they perceive as truly vertical, often with surprising error in vestibular dysfunction [3].
The interventions that come out of the workup include vestibular rehabilitation therapy (VRT, a structured set of exercises that retrain the vestibulo-ocular reflex and the postural responses), habituation training (gradual exposure to the movement patterns that destabilize you), gaze stabilization exercises, and balance retraining.
The treatment timeline varies. Many patients see measurable change within four to twelve weeks of consistent VRT. Posture often shifts as the vestibular signal recalibrates, sometimes within weeks once the upstream asymmetry is being addressed.
When PSSE alone is not enough
The structural therapy is not failing. It is being asked to overpower an upstream signal nobody is addressing.
If a patient runs a clean PSSE protocol for six to twelve months and the curve does not move, the question to ask is whether vestibular or visual asymmetry is the rate limiter. Vision and vestibular are tightly coupled. Often both are involved, with the vestibular component being the one nobody checked.
The strongest scoliosis outcomes in adult care come from a coordinated team. A PSSE-trained physical therapist. A behavioral optometrist for the visual layer. A vestibular specialist or neurologist for the vestibular layer. A myofunctional therapist for the jaw layer. The order of the team matters. Vestibular work usually belongs early, alongside vision, before the structural work fully ramps.
Find a vestibular specialist
The CSCN directory tags practitioners who address the vestibular system. Filter by Vestibular to surface vestibular rehabilitation specialists, audiologists with vestibular training, and neurologists who treat vestibular disorders.
Browse the directory filtered by Vestibular. If you have chronic head tilt, plateaued scoliosis progress, or motion-sensitivity that started or worsened in adulthood, this is often the missing variable. Pair vestibular care with visual screening and PSSE for the strongest outcomes.
FAQ
Can the vestibular system cause scoliosis?
Animal research has shown that surgically induced vestibular asymmetry in early development produces scoliotic curves with the same morphology as human adolescent idiopathic scoliosis [4]. Human studies show impaired vestibular integration in adolescents with idiopathic scoliosis compared to controls [5]. Vestibular asymmetry is not the sole cause of scoliosis in most cases, but it is a meaningful upstream contributor that should be screened.
What is vestibular rehabilitation?
Vestibular rehabilitation therapy (VRT) is a structured exercise program that retrains the vestibulo-ocular reflex, habituates the system to provocative movements, and rebuilds postural balance under different sensory conditions. It is the primary non-pharmacological treatment for vestibular dysfunction. Most VRT programs run 8 to 16 weeks.
How do I know if I have a vestibular problem?
Common signs include chronic head tilt, motion sensitivity, dizziness in low-light conditions or with eyes closed, difficulty in visually busy environments, and postural patterns (like scoliosis or chronic forward head) that have not responded to structural therapy. A vestibular assessment by a trained specialist is the definitive test.
Is vestibular dysfunction common in adults with scoliosis?
There is no large epidemiological estimate. Existing research suggests that impaired vestibular integration is more common in idiopathic scoliosis patients than in controls [5]. In adult plateau cases (cases that stopped responding to PSSE), the vestibular system is one of the most common unaddressed contributors.
Will vestibular therapy fix my scoliosis?
Vestibular therapy is not a cure for established scoliosis curves. It addresses the upstream sensory driver that may be maintaining or worsening the curve. Patients who have plateaued on structural therapy often see their PSSE work start to land differently once the vestibular asymmetry is addressed. Outcomes vary by case.
Sources
- Gagey PM, Weber B. Posturologie: Régulation et dérèglements de la station debout. 3rd ed. Masson. 2008.
- Angelaki DE, Cullen KE. Vestibular system: the many facets of a multimodal sense. Annu Rev Neurosci. 2008;31:125-150. PMID 18338968.
- Cohen HS, Sangi-Haghpeykar H. Subjective visual vertical in vestibular disorders measured with the bucket test. Acta Otolaryngol. 2018;138(2):164-167. PMID 28954574.
- Lambert FM, Malinvaud D, Glaunès J, et al. Vestibular asymmetry as the cause of idiopathic scoliosis: a possible answer from Xenopus. J Neurosci. 2009;29(40):12477-12483. PMID 19812324.
- Simoneau M, Lamothe V, Hutin E, et al. Evidence for cognitive vestibular integration impairment in idiopathic scoliosis patients. BMC Neurosci. 2009;10:102. PMID 19682367.