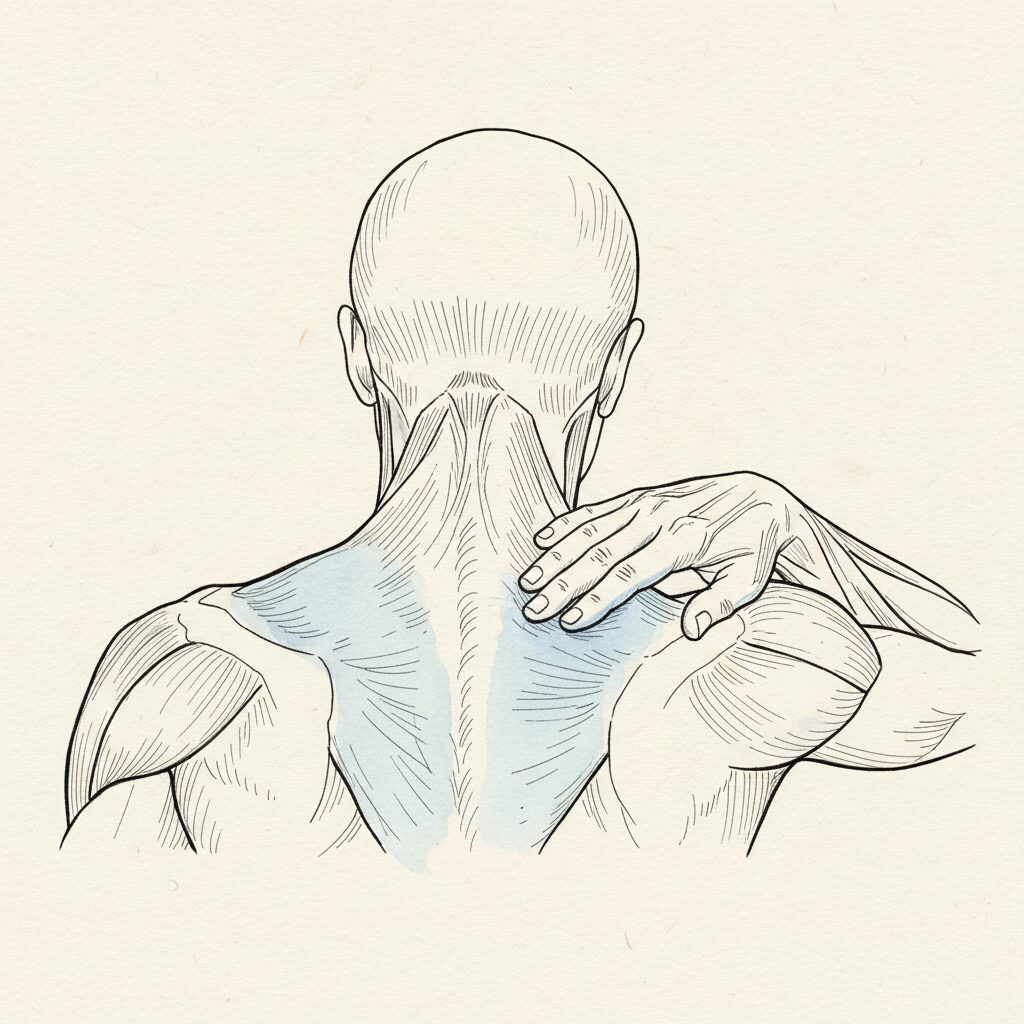
You press into your upper back and feel nothing. Not pain. Not tension. Nothing. A blank spot. A region your brain seems to have forgotten.
You assume the tissue is damaged. Dead. Beyond repair. You have had this curve long enough that the numbness feels permanent. Like that part of your body checked out years ago and is not coming back.
It is coming back. It never left. Your nervous system sealed that region. And the sealing was intelligent.
Your cortical map degraded. The tissue did not.
Your brain maintains a map of your body. Every region of your skin, every joint, every segment of your spine has a corresponding territory in your somatosensory cortex. When a region moves well and sends clear proprioceptive data, its cortical territory stays sharp. Defined. High-resolution.
When a region stops moving, stops sending signal, the map degrades. The territory blurs. Adjacent regions encroach. Neuroscientists call this cortical smudging. The brain does not delete the region. It loses the ability to distinguish it from its neighbors.
Moseley and Flor (2012) documented that chronic pain and dysfunction produce measurable reorganization of cortical body maps. The somatosensory representation of the affected region becomes less distinct, its boundaries blurring into adjacent territories. This is not tissue damage. It is representational degradation. The body part still exists, still contains intact sensory receptors, still sends afferent signals. But the cortical territory that processes those signals has lost resolution. Wand et al. (2011) demonstrated this specifically in chronic low back pain patients, showing cortical changes that correlated with the duration and severity of dysfunction. The longer the region remains in a static, low-signal state, the more the map degrades. The numb spot in your upper back is not dead tissue. It is a region whose cortical representation has lost the resolution needed to generate clear sensation.
The body sealed that region for a reason
Kyphosis places the thoracic spine in sustained flexion. The posterior tissues stretch. The anterior tissues compress. The organs beneath the curve lose space. The nervous system responds to this compression the way it responds to any region under sustained mechanical threat. It reduces signal. It dampens sensation. It seals the area.
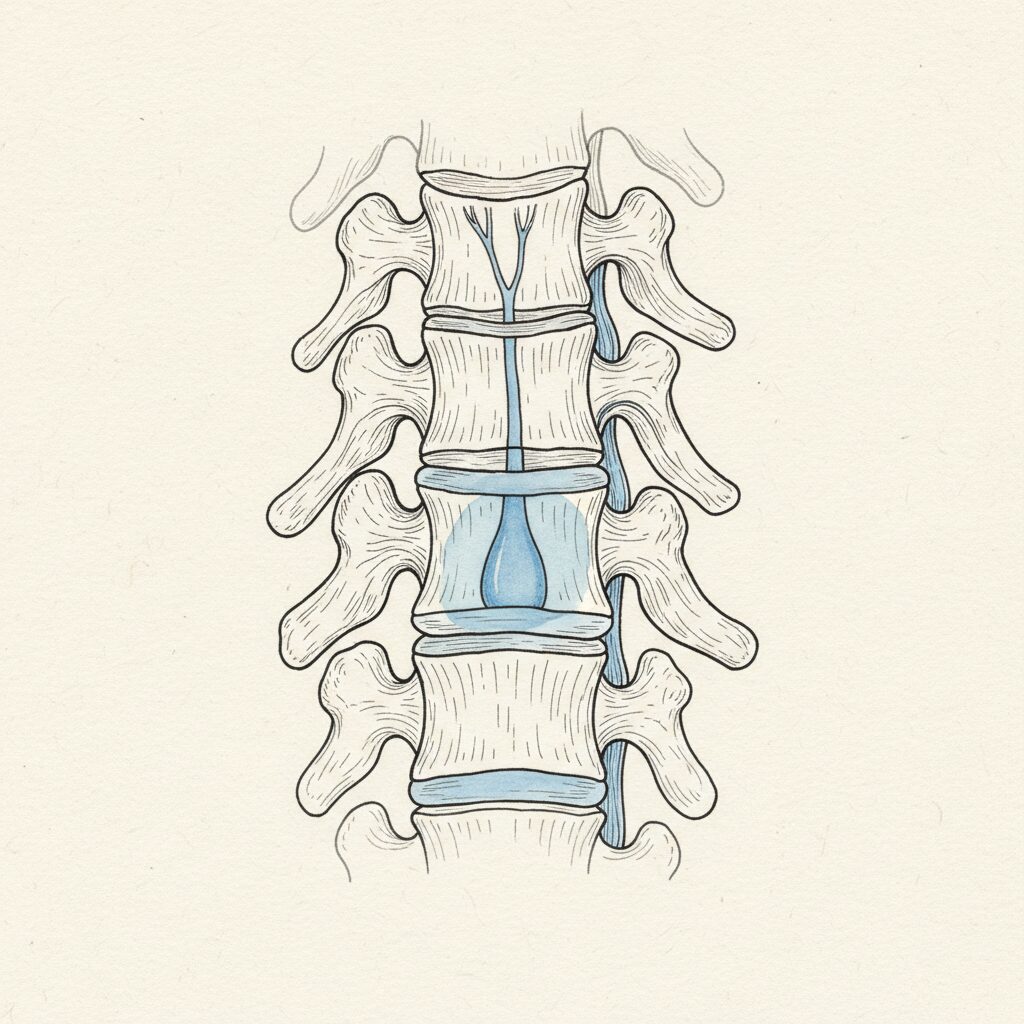
This is not failure. This is protection. The body does not numb a region by accident. It reduces sensory traffic from areas where the incoming data would generate a conflict the system cannot resolve. The sealing preserves coherence at the cost of resolution.
Levine (2010) described this pattern in trauma physiology. The body constricts around regions of overwhelm, reducing sensation and mobility to contain what it cannot yet process. The thoracic spine in kyphosis follows the same logic. The curve creates a mechanical situation the nervous system cannot resolve through movement. So it seals the region and allocates attention elsewhere.
Why trying to fix it makes it worse
Here is where most approaches fail. You notice the numb spot. You decide to fix it. You foam roll it. You have someone dig their elbow into it. You do exercises that target the area. You bring intense, corrective attention to the region.
And the numbness deepens.
Blakemore et al. (1998) established that when you generate a voluntary movement, your motor cortex sends an efference copy, a prediction of the sensory consequences of that movement. The brain uses this copy to suppress the expected sensory feedback. This is why you cannot tickle yourself. Your brain predicted the sensation before it arrived and cancelled it. The same mechanism operates when you deliberately try to “activate” or “fix” a numb region. The intention to correct generates an efference copy that suppresses the very sensory feedback you need. Corrective attention creates a prediction. The prediction gates the incoming signal. The harder you try to feel the region, the more your motor system suppresses the data that would let you feel it.
The gate opens when you arrive without fixing
Attention that carries an agenda triggers the efference copy loop. Attention that is present without demand does not.
There is a difference between “I am going to fix this numb spot” and “I am here.” The first generates a motor prediction. The second generates presence. The first suppresses incoming signal. The second keeps the sensory channel open.
When you place your awareness on the sealed region without trying to change it, the cortical map begins receiving signal it has not had. Not because you forced sensation back online. Because you stopped suppressing it. The gate was not locked from the outside. It was locked from the inside, by your own corrective intention.
The map does not rebuild in one session. Cortical reorganization takes time. But the direction is immediate. The moment you arrive without demand, the sensory channel opens a fraction wider. Signal begins returning. Resolution begins increasing. The territory in your cortex begins distinguishing that region from its neighbors again.
The numb spot was never dead. It was sealed. And sealed rooms do not open to force. They open to presence.
—
Related: Kyphosis: The Complete Guide | Why Awareness Changes Posture and Effort Doesn’t | Why Letting Go of Posture Feels Dangerous
—
“Arrive, don’t fix” is not philosophy. It is applied efference copy neuroscience. In Syntropic Core, sealed rooms open on their own timeline under autonomic safety, present-without-demand attention, and organized internal pressure. The cortical map rebuilds when signal returns. Signal returns when you stop suppressing it. See how it works.
Sources
- Moseley, G.L. & Flor, H. (2012). Targeting cortical representations in the treatment of chronic pain: a review. Neurorehabilitation and Neural Repair, 26(6), 646-652. PMID: 22331213 [T1]
Chronic pain and dysfunction degrade cortical body maps. The affected region loses representational resolution, not tissue integrity. - Wand, B.M. et al. (2011). Cortical changes in chronic low back pain: current state of the art and implications for clinical practice. Manual Therapy, 16(1), 15-20. PMID: 20655796 [T1]
Cortical reorganization in chronic low back pain correlates with duration and severity. The longer the dysfunction, the more the map degrades. - Levine, P.A. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness. North Atlantic Books. ISBN: 978-1556439438 [T2]
The body constricts around overwhelmed regions, reducing sensation and mobility to contain what it cannot yet process. Clinical model, not RCT-level evidence. - Blakemore, S.J., Wolpert, D.M. & Frith, C.D. (1998). Central cancellation of self-produced tickle sensation. Nature Neuroscience, 1(7), 635-640. PMID: 10196573 [T1]
Efference copies suppress predicted sensory feedback during voluntary action. Corrective intention toward a numb region activates the same suppression mechanism.