She did everything right
She had done five years of therapy. EMDR. Somatic Experiencing. Internal Family Systems. She could regulate. She could resource. She could name every part. Her therapist said she had done extraordinary work.
And she still could not stand up straight.
Her shoulders curled forward. Her ribs compressed on the left side. Her head sat two inches in front of her spine. She had tried yoga, Pilates, chiropractic, corrective exercise. Every practitioner gave her a different explanation and a different set of exercises. None of them asked about her nervous system. And every trauma therapist who had helped her regulate never once looked at her spine.
She fell into the gap.
The gap between two industries that treat the same body but never speak to each other. Trauma therapy on one side. Posture correction on the other. Between them, a silence where millions of people live, doing the work in both directions and watching neither one finish the job.
This article is about that gap. What lives inside it. And why closing it changes everything about how we understand posture.
Part 1: Two industries that do not talk to each other
There is a trauma industry. It is vast, growing, and doing important work. Somatic Experiencing, EMDR, polyvagal-informed therapy, IFS, trauma-sensitive yoga, breathwork, plant medicine, meditation retreats. Billions of dollars. Millions of practitioners. The central message: your body holds the record of what happened to you, and healing means completing what was interrupted.
There is a posture industry. Also vast. Chiropractic, physical therapy, corrective exercise, postural bracing, ergonomic furniture, posture apps, YouTube videos telling you to squeeze your shoulder blades. The central message: your alignment is off, and fixing it means strengthening what is weak and stretching what is tight.
Both industries are partially right. Neither one finishes the job.
The trauma world understands that the nervous system holds protective patterns. But it rarely addresses what those patterns did to the skeleton. You can complete a survival response, discharge the activation, regulate your vagal tone, and walk out of the session with the same compressed ribs and forward head you walked in with. The nervous system got the memo. The body schema did not.
The posture world understands that alignment matters. But it treats the spine as hardware. Adjust it. Brace it. Strengthen around it. This approach ignores the fact that posture is software. It is generated by a predictive model in the brain. And that model is running a program shaped by everything that ever happened to you, including the things you do not remember. External corrections get overridden by the system that generated the pattern in the first place. This is why posture correction does not work for most people.
The gap is not an oversight. It is structural. Trauma therapists are trained in nervous system regulation, not biomechanics. Physical therapists are trained in biomechanics, not trauma. The licensing, the language, the clinical frameworks, the insurance codes, the research journals, the professional conferences. All separate. The body does not care about professional boundaries. The body is one system.
Part 2: Why trauma tools alone are not enough

Let me be clear: trauma therapy saves lives. SE, EMDR, IFS, and polyvagal-informed work have helped millions of people move from survival mode toward safety. I am not criticizing these approaches. I am pointing out what they were never designed to do.
Trauma therapy regulates the nervous system. It helps you complete interrupted survival responses. It restores ventral vagal access. It builds your capacity to be present in your body without being overwhelmed. All of this is essential. None of it reorganizes your skeleton.
Here is why.
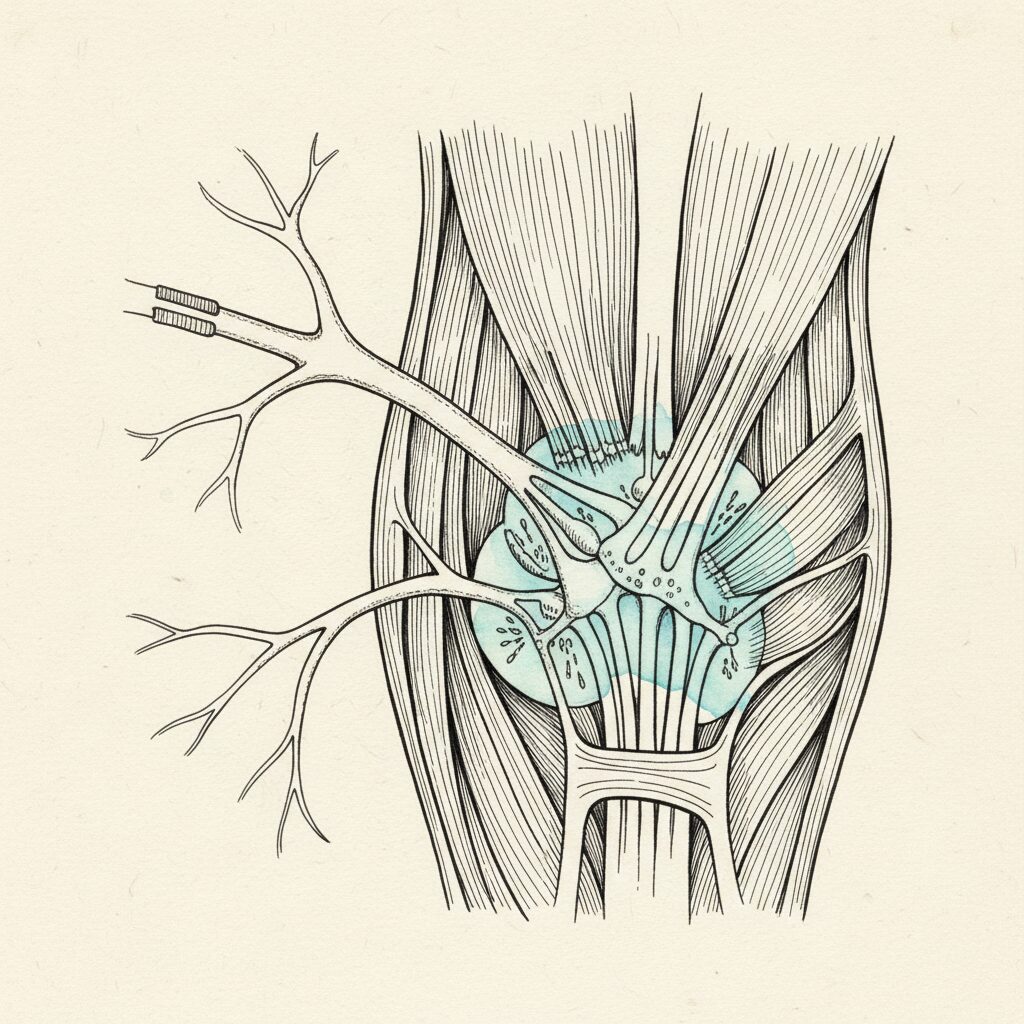
When trauma locks the nervous system in a threat state, the body adopts a defensive posture. Shoulders brace. Ribs compress. The spine shortens. The head pushes forward. This is not a metaphor. It is a motor program, executed by the brainstem, maintained by the gamma efferent system at the level of the spinal cord, below conscious awareness. The facilitatory reticular formation activates gamma motor neurons. Those neurons set the resting tension of muscle spindles. Elevated gamma drive means elevated resting muscle tone. Chronic bracing. Not because the muscles are tight. Because the brainstem set a new baseline and never released it.
This is what Thomas Hanna called sensory-motor amnesia. The cortex loses the program to release the contraction. The muscles are locked at 30 to 50 percent of their maximum contraction, and this feels like rest to the person living in the pattern. They do not know they are bracing. They cannot feel it.
Trauma therapy can resolve the autonomic activation. It can bring the nervous system out of threat mode. But the gamma efferent lock was set at the brainstem and spinal cord level. The defensive motor program was encoded into the body schema, the brain’s unconscious map of the body in space. Regulating the nervous system does not automatically rewrite the body schema. The nervous system may feel safe. The body schema still holds the shape of danger.
This is the skeleton gap.
You can pendulate. You can titrate. You can complete the survival response. You can resource. Your nervous system can shift from dorsal vagal shutdown to ventral vagal safety. And your shoulders can still be around your ears. Your ribs can still be locked. Your spine can still carry the shape of someone who never finished running.
Bessel van der Kolk wrote the book on this. Literally. The Body Keeps the Score is one of the most important books of the last decade. But even the title tells you where the work stops. The body keeps the score. It does not tell you how the body changes the score. That is the next step. And it requires a different set of tools.
If you have done trauma work and felt better emotionally but still live in a body that will not change shape, you are not failing. You finished one half of a two-part process. The other half has not been addressed yet. This is what happens after EMDR when the nervous system has resolved but the structure has not followed.
Part 3: Why posture correction alone is not enough

Now the other side.
Posture correction treats the spine as a mechanical problem. Bones are misaligned. Muscles are imbalanced. The solution: adjust the bones, strengthen the weak muscles, stretch the tight ones, brace if necessary.
This approach works for acute injuries. A torn rotator cuff needs strengthening. A stiff ankle needs mobility. For those problems, the biomechanical model is exactly right.
For chronic posture patterns, it fails. Not sometimes. Almost always. And the reason is neurological.
Your posture is not a position you hold. It is a prediction your nervous system generates, moment by moment, based on the sensory data available to it. The brain builds a model of the body in space. That model predicts what posture is necessary. The posture is the output. Not the input.
When a chiropractor adjusts your spine, the adjustment enters through proprioceptive pathways. The brain generates a motor command, predicts its sensory consequences through an efference copy, and when the predicted sensation matches the actual sensation, the signal is canceled. No prediction error. No model update. The body returns to its previous position within hours or days. The same mechanism explains why the body holds tension even after manual therapy.
When a corrective exercise program tells you to strengthen your mid-back and stretch your chest, it is targeting motor outputs. But those outputs are downstream of the prediction. The prediction was shaped by the nervous system’s threat history, its autonomic state, the quality of its sensory maps. Strengthening does not change the prediction. It just loads a pattern that was generated for protective reasons with more force.
Trying to fix a trauma posture with corrective exercise is like trying to fix a software bug by pressing harder on the keyboard.
The spine is not the problem. The spine is the printout. The operating system is the body schema. And the body schema in a trauma-organized body is running a program that says: danger is real, bracing is necessary, this shape keeps us alive.
No amount of external correction will override that program. The system will reject the update. Not because the person is not trying. Because the nervous system is running posture as a survival strategy, and survival outranks alignment every single time.
This is the nervous system gap.
Part 4: The bridge
So trauma therapy regulates the nervous system but does not reorganize the spine. Posture correction reorganizes the spine but ignores the nervous system. What sits in the gap between them?
A mechanism. Not a metaphor. A ten-step neurological chain that connects what happened to you with how you stand today.
Here is the chain:
Step 1: Threat event. Physical, emotional, developmental. It does not matter what kind. The nervous system does not distinguish between a car accident and a childhood spent in unpredictable danger. Threat is threat.
Step 2: Survival response initiated. The reticular formation in the brainstem activates fight, flight, or freeze. This is automatic. You do not choose it. It chooses you.
Step 3: Gamma efferent drive elevated. The brainstem sets a new baseline for muscle tone through the gamma motor neuron system. This is the hardware layer. Muscles are pre-tensioned for defensive action.
Step 4: Defensive motor set activated. Bracing, collapse, or asymmetric guarding. The body assumes the posture of the response it was preparing to execute. Fists clench. Shoulders rise. The spine shortens. Or the system shuts down and the body collapses forward into dorsal vagal withdrawal.
Step 5: Movement thwarted. The survival response is not completed. You could not run. You could not fight. You could not move. The response was initiated but never finished. This is what Peter Levine calls the thwarted defensive response.
Step 6: Gamma drive locked. Because the response was never completed, the reticular formation never received the signal to stand down. The elevated muscle tone becomes the new normal. The brainstem maintains it indefinitely, below cortical awareness.
Step 7: Sensory-motor amnesia develops. The cortex loses the program to release the chronic contraction. The muscles feel like they are at rest when they are at 30 to 50 percent of maximum. You cannot release what you cannot feel.
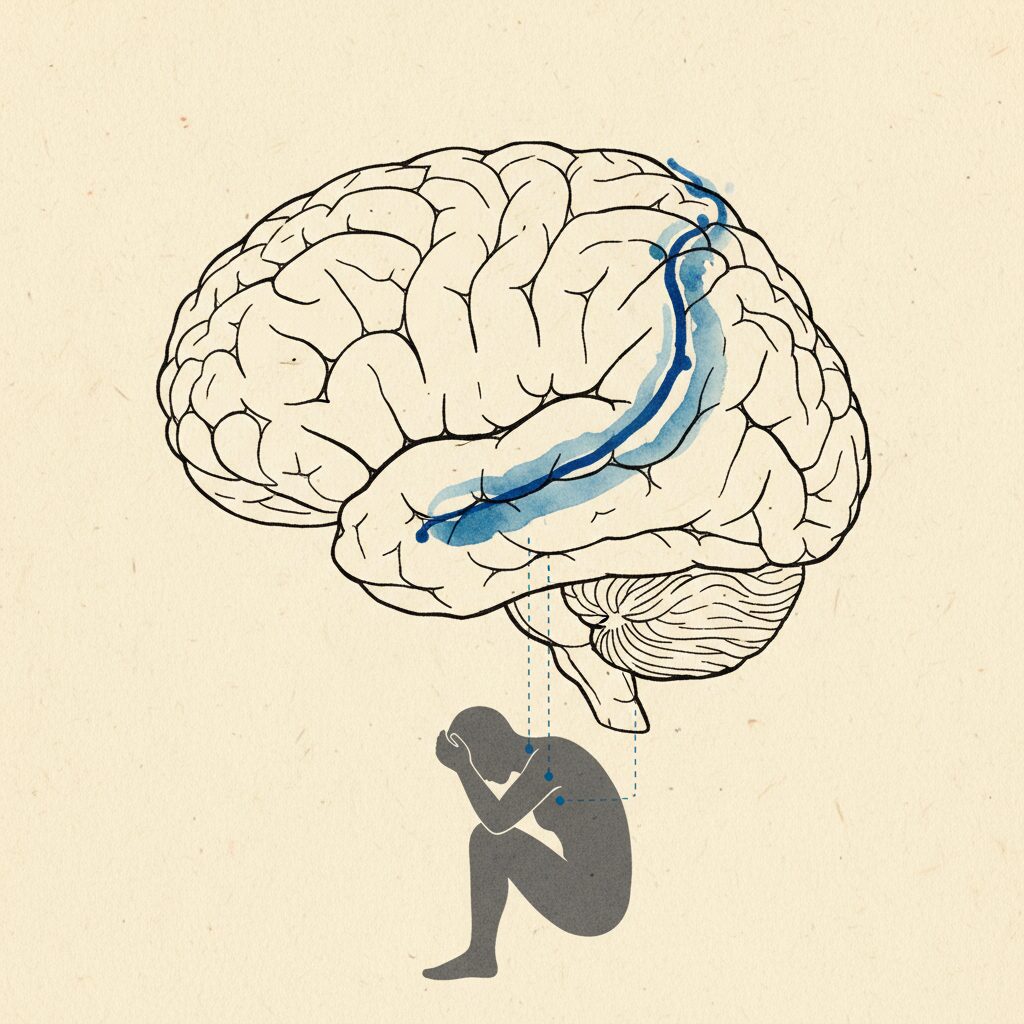
Step 8: Cortical smudging. Reduced proprioceptive input from the braced regions degrades the somatosensory maps in the brain. The body schema loses resolution in those areas. The map goes fuzzy. Then it goes dark.
Step 9: Fascial densification. Dorsal vagal shutdown reduces blood flow to the affected tissues. Hyaluronic acid aggregates in the fascial layers. The tissue thickens, stiffens, loses its sliding capacity. What was a neural lock becomes a tissue lock.
Step 10: Compensatory postural pattern. The body organizes around the regions that went offline. Other muscles compensate. Other joints take the load. The spine curves, rotates, compresses. Not randomly. Precisely. Organized around the sealed rooms, the proprioceptive dead zones where the body schema went dark.
This is the threat cascade. It is not a theory. Every step has published evidence behind it. The reticular formation’s role in postural tone. The gamma efferent system’s control of resting muscle length. Sensory-motor amnesia measured on EMG. Cortical smudging documented on fMRI. Fascial densification observed on ultrasound and histology. The chain is real. It runs in one direction, from threat to posture, and it explains why trauma lives in your posture, not as a metaphor, but as a neurological fact.
> A trauma posture is a bracing pattern the nervous system adopted during an incomplete survival response and never released, encoding threat into the shape of the spine.
This is why the two industries fail when they work alone. Trauma therapy addresses steps 1 through 6. It resolves the threat state, completes the survival response, restores ventral vagal access. But it does not address steps 7 through 10. The sensory-motor amnesia remains. The cortical smudging remains. The fascial densification remains. The compensatory pattern remains.
Posture correction addresses step 10. It tries to reverse the compensatory pattern through external force. But steps 1 through 9 are still running. The system regenerates the pattern because the upstream signals have not changed.
The bridge is working at both levels simultaneously. Resolving the nervous system state and updating the body schema. Completing the survival response and reorganizing the spine. Not one then the other. Both.
At Posture Dojo, we work at this intersection. The method uses diaphragmatic pressure to bypass the efference copy system, entering on what we call Highway 2, the interoceptive and visceral afferent pathway, rather than Highway 1, the proprioceptive-motor pathway that is locked by the gamma efferent system in trauma-organized bodies. This is why breathing exercises alone do not fix posture, but organized pressure through the five diaphragms can generate the prediction error that updates the map.
I will not teach the method in this article. That is not what this piece is for. This piece is for understanding why the gap exists and what lives inside it. The method lives inside a container, taught with safety protocols, pacing, and individual assessment. What I want you to understand right now is this: the gap is not permanent. There is a bridge. And you do not have to choose between regulating your nervous system and changing your posture. Both are necessary. Both are possible. Both happen through the same system.

Part 5: Safety before sensory before motor
There is a hierarchy to this work. Skip a step and the system rejects the update.
Safety first. The nervous system must feel safe before it will accept new information. When the system is in threat mode, it braces. The posterior chain locks. The breath shortens. The body schema freezes. No update is possible from a state of activation.
This is not a suggestion. It is a neurological constraint. The reticular formation gates sensory processing. In a threat state, the gate closes. Proprioceptive input is attenuated. Interoceptive signals are suppressed. The brain literally stops listening to the body because all resources are allocated to scanning for danger. Trying to update the body schema from a threat state is like trying to install software on a computer that is running a virus scan at full capacity. The system does not have the bandwidth.
Safety is not a warm-up. It is a prerequisite. It is the reason that every session, every practice, every interaction with the body must begin with settling the nervous system. Not as a nice gesture. As a neurological requirement.
Sensory second. Once the nervous system feels safe enough to receive information, the sensory maps must be updated. This is where cortical smudging gets addressed. Where the body schema regains resolution. Where you begin to feel parts of your body that have been offline for years or decades.
Research shows that 34 to 48 percent of chronic pain patients are alexithymic, meaning they have significantly reduced ability to identify and describe what they feel in their body. This is not a personality trait. It is a neurological consequence of prolonged threat. The sensory maps degraded. The interoceptive channels narrowed.
For this population, motor-level work is premature. You cannot update a map you cannot read. You cannot change a pattern you cannot feel. The sensory layer must come online first.
This is where practices like yoga nidra become relevant. Not as relaxation. As cortical re-differentiation. fMRI research shows that during yoga nidra body rotation instructions, subjects activate somatosensory cortex, motor cortex, and supplementary motor areas. The body schema lights up without requiring voluntary movement. For someone with extensive cortical smudging, this is a remediation protocol delivered in the form of meditation. You are systematically traversing the body map, region by region, restoring resolution to areas that went dark. This is part of how neuroplasticity actually changes posture.
Motor third. Only after safety is established and the sensory maps have regained sufficient resolution can motor patterns change. This is where the body schema actually updates. Where prediction errors generate new predictions. Where the spine reorganizes.
But motor work delivered out of order will fail. Strengthening before sensing is futile. You cannot organize what you cannot feel. Correcting before settling is counterproductive. The system interprets forced change as threat, which triggers more bracing, which makes the pattern worse. This is why posture correction does not work for trauma-organized bodies.
Safety before sensory before motor. This is the hierarchy. It is non-negotiable.
Part 6: My body, my proof
I need to tell you my story now. Not because my story is more important than yours. Because you need to know that what I am describing is not theory I read in a textbook. I lived it.
I was diagnosed with an 85-degree kypho-scoliosis at 16. An S-curve that ran the full length of my spine. The kind of curve that makes surgeons reach for the consent forms.
They told me surgery was the only option. Spinal fusion. Rods. Screws. My mother asked what would happen if we did not operate. They said I would keep getting worse. That my organs would be compressed. That my quality of life would deteriorate.
I declined the surgery. I was 16 and I was terrified, and something in me said no. I did not have a better plan. I just knew I was not ready to let someone cut my spine open and bolt it together.
What followed was 15 years of trying everything conventional. Chiropractic. Physical therapy. Corrective exercise. Yoga. Pilates. Inversion tables. Postural braces. Ergonomic everything. Some of it provided temporary relief. None of it changed the pattern. The curve remained. The compression remained. The shape of my body stayed the same no matter what I did.
I was working the problem at step 10. Trying to reverse the compensatory pattern through external force. I did not know there were nine upstream steps running the program I was trying to override.
At 33, everything collapsed. I am not going to romanticize it. It was the worst period of my life. Eight months where my body essentially stopped cooperating. Pain that made it impossible to work, to train, to function. The thing I had been managing for 17 years stopped being manageable.
What I found on the other side of that collapse was the mechanism. Not all at once. In pieces, over months of listening to a body I had spent my entire life trying to override. I found the gamma efferent lock. The sealed rooms. The compensatory patterns that were not random but precisely organized around regions where my body schema had gone dark.
And I found the bridge. The way in that did not require forcing, adjusting, bracing, or surgery. The way in through the interoceptive pathway, through organized pressure, through updating what the nervous system believed was true about my body rather than imposing what I wanted it to look like.
Eight months of focused work. Not heroic effort. The opposite. Less force. Not more. Listening before acting. Settling before sensing. Sensing before moving.
I gained two inches of height. Not from surgery. Not from stretching. From updating the body schema. From completing survival responses that had been frozen in my tissues since childhood. From restoring sensory resolution to regions of my spine that had been offline for as long as I could remember. From giving the system evidence that the old prediction was no longer accurate.
My scoliosis was never just a curve. It was the output of a body schema organized around threat. The curve was step 10. The generator was upstream. When the generator changed, the output changed.
I am not cured. That is not the word I would use. I am reorganized. My spine is still asymmetric. But the pattern is no longer driven by a locked threat state. The system is running a different program. One based on current sensory reality rather than a survival response that was never completed.
Part 7: What this means for you
If you are reading this and recognizing your own story, I want you to understand three things.
First: you are not broken. Your posture is not a defect. It is an adaptation. Your nervous system chose this shape for a reason. It was protecting you. The fact that the protection outlasted the threat does not make you damaged. It makes you a human whose body did what bodies do. It responded to threat, and the response was never completed.
Second: change is possible. The body schema is not permanent. Research from Makin and colleagues, published in Nature Neuroscience in 2025, showed that cortical body maps persist for years after amputation. The limb is gone. The map remains. If the map can persist without a body part, it can be rewritten with one. The body schema is not etched in stone. It is a living prediction, updated by sensory evidence. Change the evidence, and the prediction changes.
The cerebellum, the brain’s error-correction engine, can generate prediction errors when it receives sensory input that contradicts its current model. That is how the system updates. That is how it learns. The mechanism for change is built into the architecture. It is not something you have to create. It is something you have to access.
And for those who feel they have lost the ability to sense their own body, even that can be rebuilt. Yoga nidra, body-oriented awareness practices, and trauma-informed somatic work can restore interoceptive capacity before motor work even begins. You do not need to be able to feel your body perfectly before you start. You need to be able to feel it enough. That is a trainable skill.
Third: the order matters. You cannot skip steps. You cannot strengthen your way out of a threat state. You cannot stretch your way past a gamma efferent lock. You cannot adjust your way through cortical smudging. The hierarchy is real. Safety before sensory before motor. Work with the system, not against it.
This is what both industries miss. The trauma world works with the nervous system but stops before the skeleton reorganizes. The posture world works with the skeleton but ignores the nervous system entirely. The people who fall into the gap between them, the ones who have done the therapy and still cannot stand up straight, the ones who have tried every correction and watched it fail, they are not doing something wrong. They are missing a piece that neither industry provides on its own.
If you have done years of somatic therapy and your posture has not changed, the work was not wasted. You built the safety foundation. You completed survival responses. You restored ventral vagal access. That work is the prerequisite for what comes next. You did not fail. You finished step one.
If you have done years of posture correction and nothing holds, the exercises were not wrong. They were aimed at the wrong layer. The pattern you are trying to correct is being generated upstream of where the correction is applied. The diagnosis described a shape, not a generator. The shape is step 10. The generator is steps 1 through 9.
The connection between trauma and posture is not a metaphor. It is not poetry. It is a ten-step neurological chain that converts what happened to you into how you stand today. And every link in that chain is addressable. Not by choosing between nervous system work and structural work. By doing both, in the right order, with the right tools.
Your jaw holds the pattern. Your breath maintains it. Your sleep consolidates it. Your metabolic system pays for it. Your genes loaded the gun, but your nervous system pulled the trigger. And your nervous system can learn to put it down.
Your body never finished running. That is not a failure. That is a starting point.
The survival response that was interrupted can still be completed. The gamma efferent lock that was set at the brainstem can still be released. The cortical maps that went dark can still be illuminated. The fascial tissue that densified can still be restored. The body schema that generated a posture of protection can still generate a posture of presence.
Not through force. Not through correction. Not through trying harder.
Through evidence. Through safety. Through sensation. Through the slow, patient work of giving the nervous system new information and letting it do what it was always designed to do: update its prediction about what is possible.
—
Your body never finished running. We help it complete the run.
If this article described your pattern, you are not alone. Posture Dojo works at the intersection of nervous system regulation and structural reorganization. We do not choose between the two. We bridge them.
Join our free community and get on the waitlist for the next cohort at posturedojo.com.
—
Sam Miller is the founder of Posture Dojo and creator of the Syntropic Core method. He was diagnosed with an 85-degree kypho-scoliosis at 16, declined surgery, and spent 15 years in the gap between two industries that did not talk to each other before finding the bridge between them.