You have done the therapy. Maybe years of it. You have processed the memories. You understand the patterns. You can name what happened to you, and you can talk about it without falling apart. By every psychological measure, you have made real progress.
And your shoulders are still up by your ears.
Your breath is still shallow. Your jaw still clenches at night. Your upper back still rounds forward when you are in a room full of people. You stand in front of the mirror and you can see it: your body is still braced for something that ended years ago.
This is not a failure of therapy. It is not a failure of effort. It is a failure of target. The therapy reached your mind. It may have even reached your nervous system. But it did not reach your spine.
Trauma does not just dysregulate your emotions. It physically rewires the motor tone settings in your spinal cord and locks your body into a defensive shape. There is a specific neurological mechanism that does this, and understanding it changes everything about how you approach the problem.
“The Body Keeps the Score” Is Not a Metaphor
When Bessel van der Kolk wrote that the body keeps the score, most people interpreted it as a poetic way of saying that trauma affects the body. It is not poetic. It is literal. Trauma creates persistent physical patterns that outlast the cognitive memory of the event [1]. These patterns express as chronic muscle bracing, restricted breathing, fascial adhesion, and structural compensation.
The question is: how? What is the actual mechanism that converts a psychological experience into a physical shape?
> How does trauma physically change posture? When trauma locks the autonomic nervous system in threat mode, the reticular formation elevates gamma motor neuron drive, setting resting muscle tone at a new baseline in the spinal cord. This happens below cortical awareness. The muscles brace for a danger that no longer exists, and the cortex cannot override the setting. Over time, fascia remodels around the bracing pattern, and the temporary defensive posture becomes a permanent structural shape.
The answer lives in a system that most trauma therapists and most posture professionals have never heard of: the gamma efferent system.
The Gamma Efferent System: Where Trauma Becomes Posture
Here is the chain, step by step.
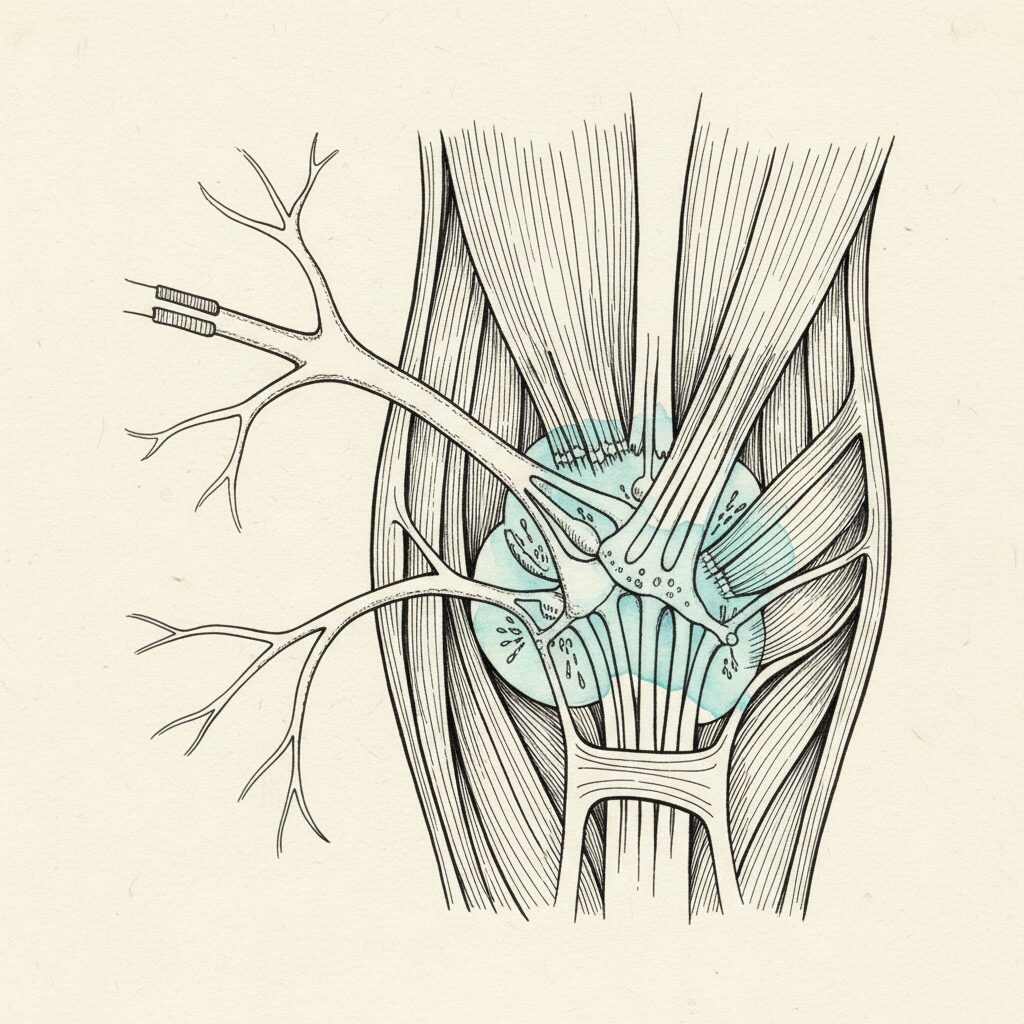
Your brainstem contains a region called the reticular formation. Among its many jobs, it controls your baseline muscle tone through a class of neurons called gamma motor neurons. These neurons do not move your muscles the way you move your arm to pick up a cup. They set the resting tension of your muscles, the background hum of tone that determines your posture when you are not thinking about your posture [3].
The gamma motor neurons control the sensitivity of muscle spindles, the tiny sensors inside your muscles that detect stretch. When gamma drive is elevated, spindle sensitivity increases. The muscle “thinks” it is being stretched even at rest, so it contracts to compensate. This creates a new resting tone, a new baseline of tension.
Here is the critical part: this entire system operates at the brainstem and spinal cord level. Your cortex, the part of your brain that thinks and decides and tries to relax, has limited authority over it.
When your nervous system detects a threat, real or perceived, the reticular formation cranks up gamma motor neuron drive. Your muscles brace. Your body prepares for impact, for flight, for fight, for collapse. This is normal. This is survival.
The problem is what happens when the threat does not resolve.
The Incomplete Survival Response
Peter Levine spent decades studying what happens when a survival response gets interrupted [2]. An animal that escapes a predator will shake, tremble, and discharge the activation before returning to baseline. The motor preparation completes its cycle. The gamma drive comes back down. The muscles release.
Humans rarely get that completion.
A child who is hit cannot fight back. A person in a car accident is strapped into a seat. Someone being yelled at in a meeting cannot run. The survival response fires, gamma drive elevates, the muscles brace for action, and then the action is thwarted. The preparatory motor set was never discharged.
Levine called these “thwarted defensive responses” [2]. Ogden and her colleagues mapped them as sensorimotor patterns that persist in the body long after the event [4]. The body is still bracing to run. Still bracing to protect the head. Still curling inward to shield the vital organs. Not because you are choosing to. Because the reticular formation never got the signal that the danger passed.
The gamma drive stays locked. The muscles stay braced. And over weeks and months and years, the fascia remodels around the bracing pattern, converting a temporary defensive posture into what looks like a permanent structural problem.
> “Gamma efferent trauma encoding is the mechanism by which unresolved threat responses become embedded in spinal cord motor tone, causing the body to maintain a defensive posture long after the danger has passed.”
Thomas Hanna measured this with EMG in the 1980s [5]. He found that chronically contracted muscles in his patients showed 30 to 50 percent of their maximum activation at rest. The patients could not feel the contraction. They had lost the cortical program for releasing those muscles. Hanna called it Sensory Motor Amnesia: the cortex literally forgets how to let go.
This is not tension you are holding. This is tension your spinal cord is holding, below the level of your awareness, in a system your conscious mind cannot directly access.
Three Postural Signatures of Trauma
Stephen Porges’ Polyvagal Theory gives us a map of how different autonomic states produce different postural patterns [3]. If you understand these three signatures, you can read trauma in a body the way a mechanic reads engine trouble.
Ventral vagal (safety and social engagement). This is the state of genuine safety. The body expresses it as extension with ease: an upright spine without effort, an open chest, a relaxed face, a voice with natural prosody. The muscles are toned but not braced. The breath moves freely. This is what posture looks like when the nervous system is not defending.
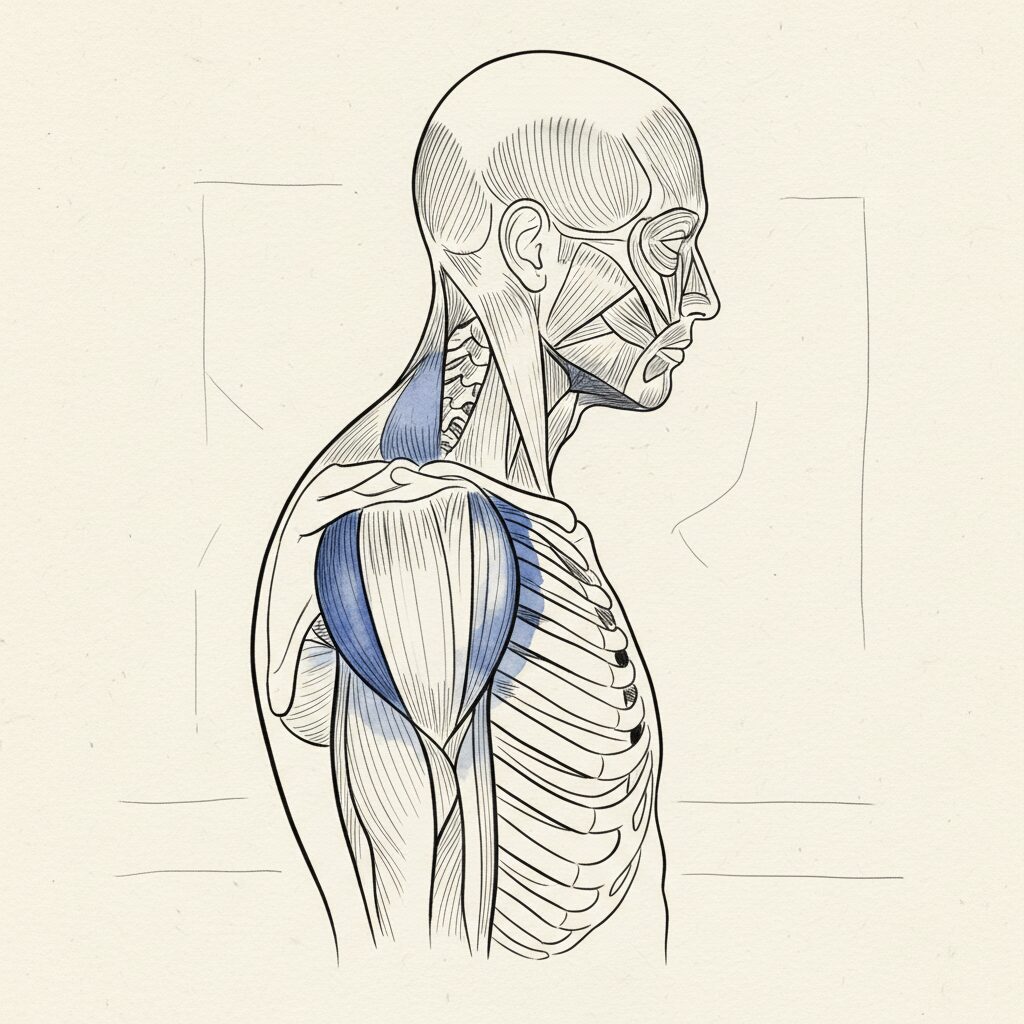
Sympathetic activation (fight or flight). When the nervous system shifts into threat mode, gamma drive elevates across the system. The body braces. Shoulders rise. The jaw clenches. The breath shortens and moves into the upper chest. The posterior chain fires to create systemic extension, a full-body stiffening that prepares for impact or rapid movement. The person looks rigid, shortened, coiled. This is the posture of someone whose body is ready to fight or run, even if they are sitting at a desk.
Dorsal vagal (freeze and shutdown). When the threat overwhelms the capacity to fight or flee, the nervous system drops into its oldest survival circuit. Muscle tone collapses. The spine rounds. The head drops forward. The breath becomes shallow and slow. The body is disappearing, making itself small, shutting down to survive what it cannot escape. This is the kyphotic, collapsed posture that many people with developmental trauma carry as their baseline.
Many people with unresolved trauma do not sit in one state. They oscillate between sympathetic bracing and dorsal collapse, between rigidity and rounding, without ever accessing ventral vagal ease. This oscillation is the autonomic signature of unresolved trauma, and it produces an alternating postural pattern that confuses practitioners who are looking for a single structural problem.
The problem is not structural. The problem is autonomic. The structure is just the output.
Why “Just Relax” Is Neurologically Impossible
This is the part that changes the conversation.
When someone tells you to relax your shoulders, drop your jaw, stand up straight, they are asking your cortex to override a brainstem-level gamma motor set. This is like asking a thermostat to override the furnace when the furnace has its own power supply. The cortex can issue the command. The brainstem can ignore it.
You can consciously relax a muscle for a few seconds. You may even hold the relaxation for a minute or two if you concentrate hard enough. But the moment your attention shifts, the gamma drive reasserts itself and the tension returns. This is not a failure of discipline. It is a neurological hierarchy. The brainstem outranks the cortex on matters of survival.
This is why:
– Stretching provides temporary relief but the tightness comes back within hours. – Massage feels great on the table but the tension returns by the next morning. – Postural cues (“shoulders back, chin tucked”) work for about thirty seconds. – Relaxation exercises calm the mind but do not change the body’s resting tone. – Even meditation, which can profoundly shift autonomic state, does not automatically reorganize the physical structure that formed around years of bracing.
The conscious mind cannot directly reprogram a gamma efferent set. This is not a limitation of your willpower. It is the architecture of the nervous system. The system that controls your resting muscle tone is not designed to take orders from the system that thinks about your resting muscle tone [5].
Four Theorists, One Mechanism
Here is something remarkable. Four of the most influential thinkers in the trauma and somatics field have been describing the same phenomenon from different angles for decades. They use different language. They come from different traditions. But when you map their observations onto the gamma efferent system, they converge on a single mechanism.
Peter Levine describes thwarted defensive responses that persist as holding patterns [2]. In gamma efferent terms: the Core Response Network activated gamma drive for a survival action that was never completed, and the drive never came back down.
Bessel van der Kolk describes muscles braced for impact that will not release during relaxation [1]. In gamma efferent terms: the brainstem maintains elevated tone independent of cortical commands, which is exactly what happens when the reticular formation is locked in threat mode.
Thomas Hanna describes Sensory Motor Amnesia, a 30 to 50 percent chronic contraction that the person cannot feel and cannot release [5]. In gamma efferent terms: elevated gamma baseline resets what “rest” feels like, and the cortex loses the release program for those muscles.
Stephen Porges describes postural signatures of different vagal states, bracing in sympathetic activation, collapse in dorsal vagal shutdown [3]. In gamma efferent terms: the autonomic circuit drives the reticular formation, which drives gamma motor neurons, which drive the postural pattern.
All four are describing different views of the same hardware. The gamma efferent system is the bridge that converts autonomic state into postural shape. It is the mechanism that makes “the body keeps the score” a literal, measurable, neurological fact.
The Master Chain: From Threat to Structure
When you line up the full sequence, the path from trauma to chronic posture becomes clear:
1. Threat event occurs (physical, emotional, or developmental). 2. Survival response initiates via the reticular formation (fight, flight, or freeze). 3. Gamma efferent drive elevates, setting a new muscle tone baseline at the brainstem level. 4. Defensive motor set activates: bracing, collapse, or asymmetric guarding. 5. Movement is thwarted: the survival response does not complete. 6. Gamma drive locks: the reticular formation maintains the elevated tone indefinitely. 7. Sensory Motor Amnesia develops: the cortex loses the ability to release the contraction. 8. Proprioceptive input degrades: reduced movement reduces the quality of the body map. 9. Fascia remodels: tissue densifies around the bracing pattern, converting a neuromuscular holding into a structural change. 10. Compensatory posture emerges: the rest of the body reorganizes around the locked pattern.
Step 10 is what you see in the mirror. But the cause is at step 2, and the lock is at step 6. Everything after step 6 is downstream consequence.
This chain was recently supported by the first direct measurement of dissociation affecting postural sway [7]. Papadopoulos and colleagues showed that trauma-experienced individuals with dissociative symptoms demonstrate measurably different postural control, providing the first quantitative evidence that autonomic trauma states alter the body’s physical organization in real time.
The Gap That Nobody Talks About
Here is the part that matters most if you are someone who has done trauma work and still lives in a body that has not changed.
The best trauma therapies in the world, Somatic Experiencing, EMDR, IFS, sensorimotor psychotherapy, are designed to regulate the autonomic state. And they work. They help the nervous system shift out of chronic threat mode. They complete the interrupted survival responses. They restore ventral vagal access. This is profound, life-changing work.
But here is the gap: autonomic regulation does not automatically reorganize the physical structure.
The nervous system gets the memo. The spine does not.
By the time someone has carried a trauma-organized posture for years or decades, the problem is no longer purely neurological. The fascia has remodeled. The proprioceptive map has degraded. The body schema, the brain’s internal model of the body, has reorganized around the compensation. Even when the gamma drive finally comes down, the structural changes remain. The tissue is denser. The body map is blurred. The compensatory patterns have become the body’s new normal.
This is why your body holds tension even after successful trauma therapy. It is why people who have done beautiful, deep therapeutic work still carry the posture of the person they were before the healing. The therapy changed the signal. But the tissue had already remodeled around the old signal, and tissue does not automatically remodel back.
This is not a criticism of trauma therapy. It is a recognition that trauma affects the body at two levels, and most approaches only address one:
Level 1: The autonomic signal. The nervous system locked in threat mode, driving gamma efferent tone upward. Trauma therapies address this level. They work.
Level 2: The structural remodeling. The fascia, proprioception, and body schema that reorganized around the bracing pattern. This level requires physical intervention that can reach below cortical awareness and restore the tissue itself.
If you address Level 1 without Level 2, the nervous system calms but the body stays locked. If you address Level 2 without Level 1, the tissue softens but the nervous system braces it right back up. Both levels need to be addressed, in the right order.
This is the conversation that needs to happen between the trauma therapy world and the movement/posture world. Not as competing approaches, but as two halves of a single process. The therapist handles the signal. The body worker handles the structure. Neither alone is sufficient.
What This Means for You
If you recognize yourself in this article, if you have been carrying a posture that feels like it belongs to a younger, more frightened version of you, here is what I want you to know.
You are not broken. You are not lazy. You are not failing at posture. Your body organized itself around a threat it could not escape, and it did so using a system that operates below your conscious awareness. That organization was intelligent. It was protective. And it is no longer serving you, but it will not undo itself just because you understand it intellectually.
Understanding the mechanism matters because it changes what you try. You stop blaming yourself for not being able to relax. You stop doing exercises that target the symptom (the rounded shoulders, the forward head) while ignoring the cause (the brainstem-level gamma set that is producing the posture as an output). You start looking for approaches that can reach below cortical awareness, that can address the tissue where the pattern lives, not just the mind that remembers it.
If you have done trauma therapy, that work is not wasted. It is foundational. The nervous system regulation you built is the prerequisite for the structural work to hold. Without it, any physical change would get overwritten by the next threat response. With it, the body has a chance to reorganize around a new signal, one that says the danger has passed, and the bracing can finally stop.
The full threat cascade maps every step of this chain in detail, if you want the complete mechanism.
The Bottom Line
Trauma does not just live in your memories. It does not just live in your nervous system. It lives in your muscle tone, set by gamma motor neurons in your spinal cord, maintained by a brainstem that never got the all-clear signal. It lives in fascia that remodeled around years of bracing. It lives in a body map that blurred from years of reduced movement. It lives in a posture that was built to protect you and became the shape you carry through the world.
The body keeps the score. The score is written in your resting muscle tone, your fascial density, your proprioceptive map, and the shape of your spine.
Reaching it requires reaching below the level of conscious thought, below the cortex, below the cognitive mind that has already done its work. It requires reaching the tissue where the pattern actually lives.
Trauma does not just live in your mind. It lives in your muscle tone. And we know how to reach it.
—
If you want to understand the specific mechanism that keeps your body locked in tension, read The Threat Cascade. If you have done EMDR or somatic therapy and your posture has not changed, read Posture Integration After EMDR. If you want to understand why your body holds tension in the first place, start with Why Your Body Holds Tension.
Ready to address trauma where it actually lives? Join the newsletter for the neuroscience of posture, trauma, and structural change. If you are a therapist interested in bridging autonomic regulation and postural reorganization, visit our therapist partnership page.
—
References
1. Van der Kolk, B. (2014). The Body Keeps the Score. Viking. 2. Levine, P. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness. North Atlantic Books. 3. Porges, S.W. (2011). The Polyvagal Theory. W.W. Norton. 4. Ogden, P., Minton, K. & Pain, C. (2006). Trauma and the Body: A Sensorimotor Approach to Psychotherapy. W.W. Norton. 5. Hanna, T. (1988). Somatics: Reawakening the Mind’s Control of Movement, Flexibility, and Health. Da Capo Press. 6. Payne, P., Levine, P. & Crane-Godreau, M. (2015). Somatic experiencing: using interoception and proprioception as core elements of trauma therapy. Frontiers in Psychology, 6, 93. 7. Papadopoulos, N. et al. (2024). Postural Responses in Trauma-Experienced Individuals. Biomedicines, 12(12). 8. Nummenmaa, L. et al. (2014). Bodily maps of emotions. PNAS, 111(2), 646-651. 9. Herrera, E. et al. (2025). Impaired interoception in Colombian victims of armed conflict with PTSD. Frontiers in Psychology.
Sources
- Van der Kolk, B. (2014). The Body Keeps the Score. Viking. [T2]
Trauma stored as persistent physical patterns in muscle tone and breathing. - Levine, P. (2010). In an Unspoken Voice: How the Body Releases Trauma and Restores Goodness. North Atlantic Books. [T2]
Thwarted defensive responses persisting as chronic holding patterns. - Porges, S.W. (2011). The Polyvagal Theory. W.W. Norton. [T1]
Autonomic state hierarchy, neuroception, postural signatures of vagal state. - Ogden, P., Minton, K. & Pain, C. (2006). Trauma and the Body: A Sensorimotor Approach to Psychotherapy. W.W. Norton. [T2]
Sensorimotor processing of trauma, defensive motor patterns. - Hanna, T. (1988). Somatics: Reawakening the Mind’s Control of Movement, Flexibility, and Health. Da Capo Press. [T1]
Sensory Motor Amnesia, chronic subcortical contraction, EMG evidence. - Payne, P., Levine, P. & Crane-Godreau, M. (2015). Somatic experiencing: using interoception and proprioception as core elements of trauma therapy. Frontiers in Psychology, 6, 93. [T2]
Core Response Network, interoception and proprioception in trauma recovery. - Papadopoulos, N. et al. (2024). Postural Responses in Trauma-Experienced Individuals. Biomedicines, 12(12). [T2]
First direct measurement of dissociation affecting postural sway. - Nummenmaa, L. et al. (2014). Bodily maps of emotions. PNAS, 111(2), 646-651. [T1]
Emotions produce topographically distinct bodily sensation maps across cultures. - Herrera, E. et al. (2025). Impaired interoception in Colombian victims of armed conflict with PTSD. Frontiers in Psychology. [T2]
Trauma disrupts the ability to read the body’s own signals.
Comments
One response to “Why Trauma Lives in Your Posture (Not Just Your Mind)”
[…] trauma lives in your posture […]