You have kyphosis. You also have tinnitus. You have been treating them as two separate problems, seeing two separate specialists, doing two separate sets of exercises. Nothing has worked for either one.
They are not two problems. They are two outputs of the same predictive model.
The compensation chain
Thoracic kyphosis increases the forward curvature of your upper back. Your body has one non-negotiable requirement: horizontal gaze. Your eyes must face forward. So the cervical spine compensates. It extends to bring your head back over your shoulders and your eyes to the horizon.
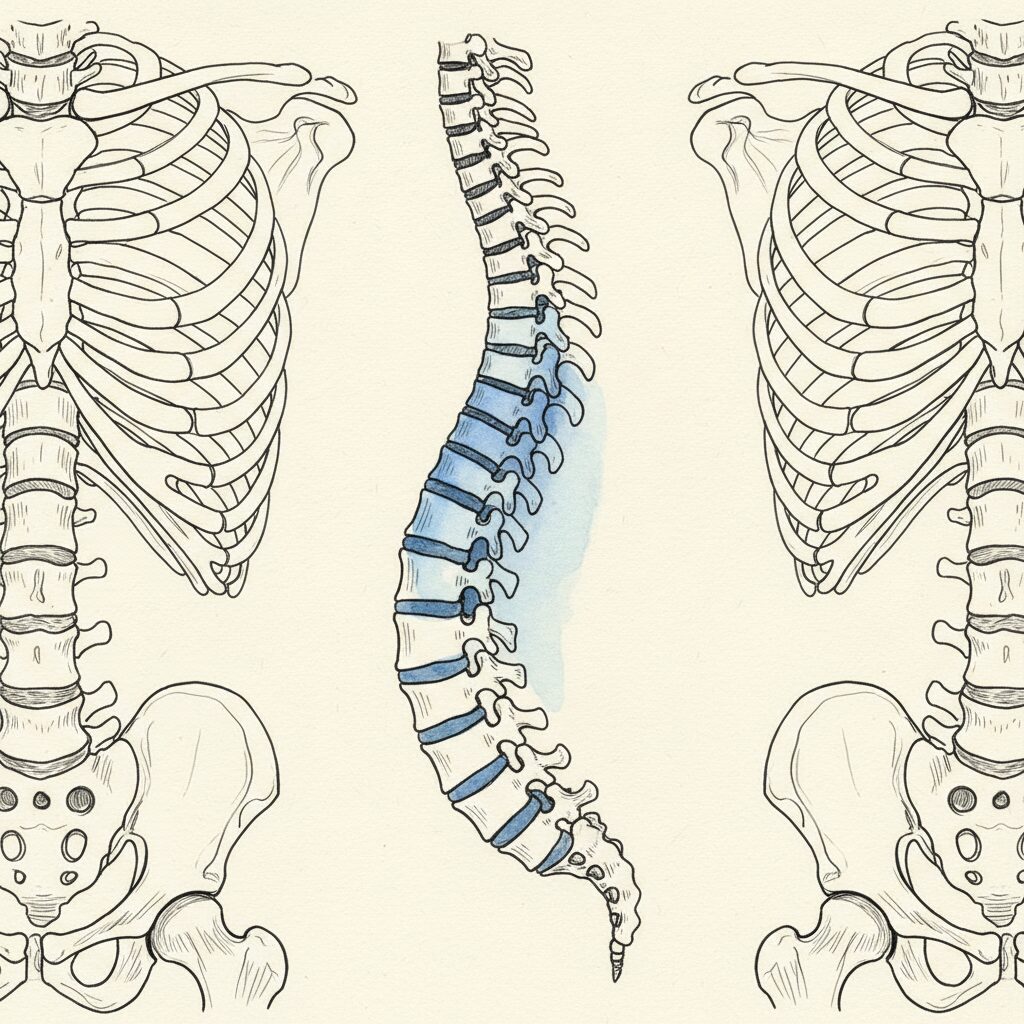
This is not a choice. It is an automatic postural adjustment driven by the vestibular and visual systems. Harrison et al. (2005) modeled this relationship mathematically: sagittal thoracic curvature directly predicts compensatory cervical lordosis [3]. More thoracic kyphosis, more cervical extension. The geometry is deterministic.
Cervical extension compresses the suboccipital triangle. The four small muscles at the base of your skull, dense with proprioceptors, rich with connections to the dura mater and the vertebral artery. Biondi (2005) documented how suboccipital compression alters vertebral artery hemodynamics and generates referred pain patterns throughout the head and face [1].
This is where the tinnitus enters.
Where sound meets structure
The dorsal cochlear nucleus processes auditory signals. It also receives somatosensory input from the upper cervical spine and the trigeminal nerve. This is not a design flaw. It is integration. The brain uses head and neck position to calibrate auditory processing.
Michiels et al. (2016) conducted a systematic review demonstrating that cervical physiotherapy produces measurable improvements in tinnitus loudness and distress in patients with cervicogenic somatic tinnitus. The mechanism: upper cervical dysfunction alters somatosensory input to the dorsal cochlear nucleus, which modulates auditory processing. When cervical mechanics normalize, the aberrant somatosensory signal resolves, and the tinnitus decreases. This is not a pain phenomenon. It is a signal processing phenomenon. The cochlear nucleus is receiving bad data from a compressed cervical spine, and it generates a phantom auditory signal from that bad data. Fix the cervical input, and the phantom signal attenuates [2].
Your tinnitus is not in your ears. It is in your neck. And your neck problem is not in your neck. It is in your thoracic spine. And your thoracic spine is not generating kyphosis because of weak muscles. It is generating kyphosis because of a predictive model that has not updated.
One prediction, two symptoms
The nervous system runs one model. That model generates thoracic kyphosis as an output. The kyphosis forces cervical extension. The cervical extension compresses the suboccipital triangle. The compression alters somatosensory input to the dorsal cochlear nucleus. The cochlear nucleus generates a phantom auditory signal.
Kyphosis and tinnitus. Two symptoms. One prediction.
Porges (2011) described how the autonomic nervous system governs the middle ear muscles through the vagal system. In a sympathetically dominant state, the tensor tympani and stapedius alter their tension, shifting auditory processing toward threat-relevant frequencies and away from human voice range [4]. Chronic thoracic kyphosis is itself a sympathetic posture, a protective flexion pattern that signals threat to the autonomic system. The tinnitus is not just a mechanical consequence of cervical compression. It is also an autonomic consequence of a nervous system running in a defensive state. The ringing is the sound of a system on alert.
Why treating them separately fails
The ENT finds nothing wrong with your ears. Hearing tests are normal. You are told to habituate. The orthopedist sees the kyphosis and prescribes extension exercises. You do them for months. Neither specialist knows about the other problem. Neither intervention addresses the shared upstream cause.
Cervical exercises alone fail because they address the compensation, not the driver. The cervical spine is extending because it has to. As long as the thoracic prediction persists, cervical extension will regenerate. And the tinnitus will persist with it.
The exit is not at the neck. It is not at the ear. It is at the prediction.
—
Related: Kyphosis: The Complete Guide | TMJ and Posture: The Jaw Connection | Scoliosis and Breathing Problems
—
Syntropic Core Reset addresses the thoracic prediction. As it updates, compensatory cervical extension is no longer necessary. Craniocervical compression resolves because the upstream prediction changed. Syntropic principle: restore regulation at the center, and organization ripples outward. See how it works.
Sources
- Biondi, D.M. (2005). Cervicogenic headache: a review of diagnostic and treatment strategies. Journal of the American Osteopathic Association, 105(4 Suppl 2), 16S-22S. PMID: 15928349 [T1]
Suboccipital compression alters vertebral artery flow and generates referred craniofacial symptoms. - Michiels, S., et al. (2016). Does multi-modal cervical physical therapy improve tinnitus in patients with cervicogenic somatic tinnitus? Manual Therapy, 26, 177-183. PMID: 27507590 [T1]
Cervical PT improves tinnitus by normalizing somatosensory input to the dorsal cochlear nucleus. - Harrison, D.E., et al. (2005). Modeling of the sagittal cervical spine as a method to discriminate hypolordosis. Spine, 29(22), 2485-2492. PMID: 15543059 [T1]
Sagittal thoracic curvature mathematically predicts compensatory cervical lordosis. - Porges, S.W. (2011). The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation. W.W. Norton. [T1]
Autonomic state governs middle ear muscle tension and auditory processing. Defensive states shift auditory perception.
Comments
One response to “The Kyphosis-Tinnitus Connection: Why Your Body Didn’t Create Two Separate Problems”
[…] Related: The Complete Guide to Kyphosis | The TMJ-Posture Connection | Tech Neck Is an Eye Problem | The Kyphosis-Tinnitus Connection […]