The best scoliosis exercises do not look like exercises at all.
They look like a person lying on the floor, barely moving, paying attention to something invisible. No reps. No sets. No sweat. If you walked into the room you might think nothing was happening.
Everything is happening. It is just happening at a layer most fitness models do not acknowledge exists.
The Layer Underneath the Muscles
Conventional physical therapy for scoliosis works through the muscular system. Strengthen the weak side. Stretch the tight side. Mobilize restricted joints. Push the curve toward symmetry using external force and muscular effort.
Somatic approaches work through the sensory system. They do not push the body into a new position. They update the nervous system’s perception of where the body is. The distinction sounds subtle. It is the difference between rearranging pixels on a screen and rewriting the code that generates the image.
Somatic methods share a core principle: the body’s shape is generated by the nervous system’s internal map. Change the map, and the muscles reorganize automatically. Force the muscles without changing the map, and the map reasserts the original pattern the moment the force is removed.
Kami, one of our participants, described this from the inside: “I started noticing my diaphragm holding throughout the day. I’d bring awareness there and it just wasn’t moving. And then allowing it to move was less force. Not more.”
Less force. The body did not need to be pushed into the right shape. It needed to be allowed to find it.
Feldenkrais: Awareness Through Movement
Moshe Feldenkrais was a physicist, judo black belt, and engineer who developed his method after a severe knee injury. His insight: the nervous system controls movement through internal representation, not muscle commands. If the representation is distorted, movement will be distorted. Correct the representation, and movement corrects itself.
Feldenkrais lessons use slow, small, unusual movement patterns to give the nervous system new sensory information. The movements do not build strength or increase flexibility. They provide the body schema with data it has not encountered before.
For scoliosis, this matters because the body schema has consolidated around the curve. The nervous system’s map includes the rotation, the asymmetry, the restriction. It does not perceive these as abnormalities. It perceives them as normal. The schema has adapted to the curve so thoroughly that the person cannot feel their own asymmetry from the inside.
Feldenkrais lessons introduce movement variations the schema does not predict. A rotation in an unexplored direction. A weight shift the habitual pattern does not include. A breathing pattern the rib cage has not attempted. Each creates a small prediction error. The schema expected one thing. It received another.
Maps update through prediction errors.
Alexander Technique: Inhibition and Direction
Frederick Matthias Alexander was an actor who lost his voice during performance. Years of self-observation in mirrors revealed that the way he used his body during speech was causing the vocal problem. Two principles emerged: inhibition (pausing habitual reactions) and direction (gentle intention toward length and expansion without effort).
Alexander Technique does not prescribe exercises. It addresses the habitual pattern of use that generates the shape. The teacher works through gentle hands-on contact, guiding the system toward different organization without forcing a new position.
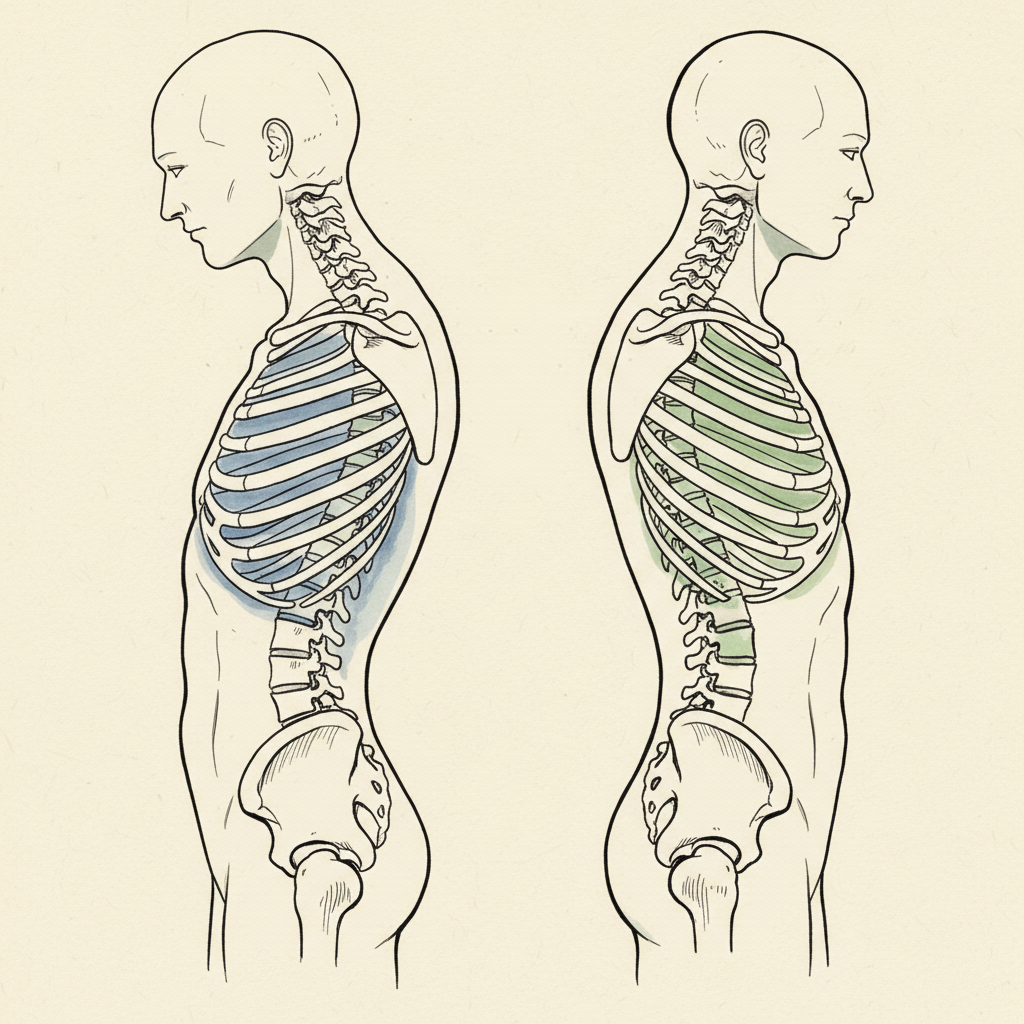
For scoliosis, Alexander highlights something exercise programs miss: the curve is maintained, in part, by habitual movement patterns the person does not know they are performing. How they sit. How they reach. How they breathe. How they turn their head. Every movement carries the signature of the scoliotic pattern. The curve is not just a shape the spine holds. It is a shape the person recreates, unconsciously, in every action.
The method helps the person become aware of these patterns and learn to stop performing them. Not by trying harder. By doing less.
Hanna Somatics: What Sensory Motor Amnesia Means
Thomas Hanna coined the term “sensory motor amnesia.” Muscles chronically contracted. The person has lost the ability to voluntarily release them. The muscles are fine. The nervous system has forgotten that releasing them is an option.
Pandiculation: consciously contract a chronically held muscle, then slowly and deliberately release it. The sequence re-engages cortical control. The nervous system remembers it can let go.
In scoliosis, sensory motor amnesia is pervasive. Muscles on the concave side are chronically shortened. The person cannot release them voluntarily. May not even be aware of the contraction. The body schema has incorporated it as baseline. Invisible from the inside.
Continuum Movement: The Fluid Layer
Emilie Conrad developed Continuum from her study of Haitian dance. The body is primarily fluid. Continuum uses breath, sound, and micro-movements to access layers that conventional exercise cannot reach.
For scoliosis, it offers access to visceral and fascial layers that the other methods do not touch. The curve is not just muscular and skeletal. Fascial patterns span the entire torso. Organ positions have adapted to the rotated rib cage. Fluid dynamics have reorganized around the asymmetrical container. Continuum’s micro-movements create possibility in tissue that has been static for years.
The most unconventional of the four. Also the most humbling. The work is extremely slow, internally generated, and follows the body’s own fluid dynamics. Control dissolves. Listening replaces effort.
The Real Difference Between Somatic and Conventional
People ask: which works better? Feldenkrais or physical therapy? Alexander or Schroth?
Different layers of the same problem.
Physical therapy addresses the muscular and biomechanical layer. Changes tissue length, builds strength, improves joint mobility. Real changes. They matter. But they operate at the output layer.
Somatic approaches address the neural layer. How the nervous system perceives and organizes the body. They update the map that generates the muscular pattern. These changes often feel more durable because they operate at the source rather than the expression.
Laura, who came to our work with a Feldenkrais and Hanna background, described the difference: “I feel like I’ve increased the awareness of my body so I can tell where my posture is compromised, but I don’t yet have the tools or the path to make the changes.”
Awareness without tools. That is the ceiling of general somatic work applied to scoliosis. Feldenkrais is a general method. Alexander is a general method. Neither was designed specifically for the rotated, asymmetrical, compressed architecture of a scoliotic spine. A Feldenkrais teacher who does not understand scoliosis-specific mechanics may improve body awareness without touching the rotational patterns that maintain the curve.
Schroth and Somatic Work Are Not Competitors
Schroth is the most established scoliosis-specific exercise method. Rotational breathing, specific postural corrections, three-dimensional deformity addressed directly. Biomechanically sophisticated. Works at the tissue level.
Alexander works at the neural level. No scoliosis-specific exercises. Addresses habitual patterns of use that maintain the curve.
The plumber and the architect. One fixes the pipes. The other designs the building. You need both, but they are solving different problems.
Laura again, comparing directly: “With the Schroth, I only ever really got control of my ribs there. With the pressure, I was able to actually feel the imbalances in the pelvis for the first time.”
Schroth without sensory updating produces corrections that wash out. Somatic work without scoliosis-specific mechanical tools produces awareness without application.
What I Took from Each
Twenty years with my own curve across every modality available.
The somatic principle is correct. Update the map, not the muscles. The body schema is the source. Sensory input is the medium of change. Without this foundation, every correction is temporary.
But the somatic methods applied generically are not specific enough for scoliosis. The rotated rib cage. The asymmetrical diaphragm. The compressed vagal pathway. The self-reinforcing loop between curve, breath, and nervous system state. These require specific understanding that general somatic education does not provide.
The approach I use takes the somatic principle and applies it inside a scoliosis-specific framework. Safety first: reduce the threat state. Sensory second: restore inputs starting with the highest-weighted ones, working down. Motor third: the specific exercises, the rotational breathing, the pressure restoration, the ground contact. All of it organized by the nervous system’s own hierarchy.
Pattern first. Strength second. Most programs reverse the sequence.
The Map Is the Starting Point
If you have scoliosis and you have hit a ceiling with conventional approaches, the somatic world offers a different starting point. Not a better exercise. A different layer. The sensory system instead of the muscular system.
But choose practitioners who understand scoliosis specifically. The general principle is necessary. It is not sufficient.
The muscles do what the map says. Change the map.
Sam Miller is the founder of Posture Dojo. He lives inside an 85-degree kyphoscoliosis and has for thirty years. He writes from the inside of that experience.
Syntropic Core Reset
Most posture programs give you exercises. This one updates the system that generates your posture. Four weeks live with Sam Miller. You learn how the hidden map works, why everything else missed it, and how to give your nervous system the evidence it needs to generate a different pattern. Breath. Ground contact. Safety. Sensory input. Floor to standing. You leave with a daily practice that holds because the map itself has changed.
Limited spots. Next cohort enrolling now.
Details and enrollment →
Comments
One response to “Somatic Exercises for Scoliosis: Feldenkrais, Alexander Technique, and What They Share”
[…] Somatic exercises address the sensory layer but often stop there. The map updates. The person feels more. What they frequently lack is the organized pressure that gives the new map something structural to build on. Awareness without hydraulic support is insight that does not accumulate. […]