This article is for the person sitting with a surgical recommendation. Not hypothetically. Actually sitting with it. A Cobb angle above 40 or 50 degrees. A curve that has progressed despite years of bracing, physical therapy, observation. A surgeon who says the time has come.
This is not an anti-surgery article.
Spinal fusion is a real intervention that produces real structural correction. The data supports it. The surgeons who perform it are solving a problem within the model they were trained in. And for some people, at some curve severities, it is the right decision.
But there is a gap between what surgery addresses and what generates the curve in the first place. That gap is not discussed in most surgical consultations. Not because the surgeons are hiding it. Because the model they are operating within does not include it.
This article exists to close that gap. So the decision you make is fully informed. Not just structurally informed. Systemically informed.
Medical disclaimer: This article is educational. It is not medical advice. It does not replace consultation with your orthopedic surgeon or medical team. Every surgical decision involves individual factors that only your treating physicians can assess. The information here is intended to support your understanding, not to direct your decision.
What spinal fusion actually does
Spinal fusion for scoliosis is a well-established surgical procedure. It has been refined over decades. The goal is straightforward: mechanically reduce the curve and prevent further progression at the fused segments.
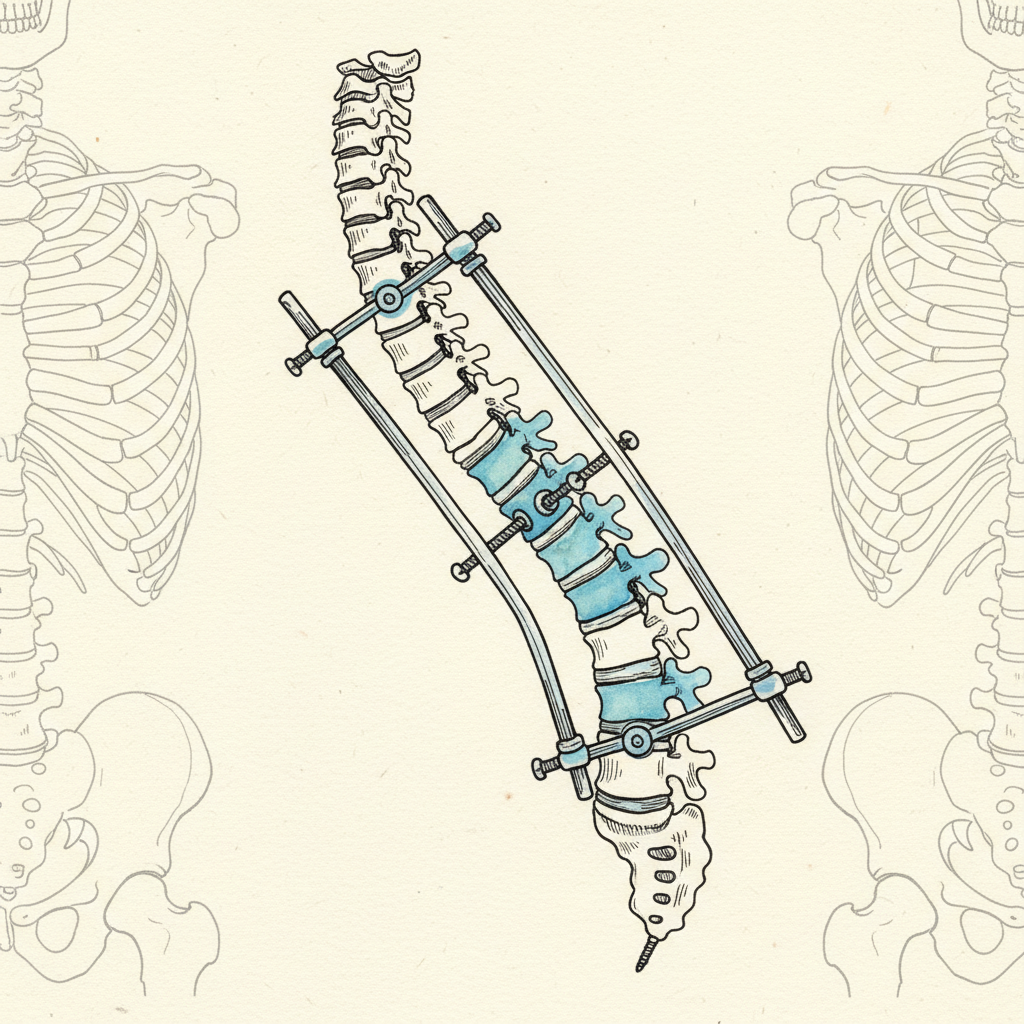
Here is what happens. The surgeon exposes the vertebrae along the curve. Metal rods are attached to the spine using pedicle screws. The rods are contoured to a corrected position and the vertebrae are drawn toward that position. Bone graft material is placed along the instrumented segments to promote fusion. Over months, the vertebrae fuse into a single bony mass. The curve is mechanically fixed in its corrected position.
The Lenke classification system guides surgical planning by categorizing curves into six types based on the location and flexibility of the structural and compensatory curves [1]. This determines which segments to fuse and which to leave mobile.
Typical correction ranges from 50 to 70 percent curve reduction [1]. A 60-degree curve corrected to 20 or 25 degrees. That is significant structural change. It is real. It is measurable on post-operative imaging.
The Weinstein 2013 study in the New England Journal of Medicine, while focused on bracing outcomes for adolescent idiopathic scoliosis, confirmed the broader finding that curves above surgical threshold progress without intervention [2]. Fusion stops that progression at the instrumented levels. Completely.
This is what fusion does well. It arrests progression. It reduces the curve. It changes the structural shape of the spine at the fused segments.
Spinal fusion for scoliosis mechanically corrects the spinal curve by attaching metal rods and pedicle screws to the vertebrae along the curve, then promoting bony fusion of those segments. The Lenke classification system (Lenke et al. 2001) guides surgical planning by categorizing scoliosis curves into six types. Typical correction achieves 50-70% curve reduction. The Weinstein 2013 NEJM study on adolescent idiopathic scoliosis confirmed that curves above surgical threshold progress without intervention. Fusion eliminates motion at the instrumented segments and prevents further curve progression at those levels. It is one of the most well-established spinal procedures, with decades of refinement in technique and instrumentation.
What fusion cannot do
Fusion changes the structure. It does not change the system that generated the structure.
Your brain maintains an internal model of your body called the body schema [3]. This model runs below conscious awareness. It generates your posture as a continuous prediction based on decades of sensory input. The lateral curve in your spine is one output of that prediction.
Fusion corrects the output at the fused segments. The rods and screws hold the vertebrae in their new position. But the body schema that generated the original curve is still running. The prediction has not been updated. The generator has not been addressed.
This matters for two reasons.
First, the unfused segments above and below the fusion still receive instructions from the same prediction model. The brain’s body schema does not stop generating output at the segments adjacent to the fusion. It adapts. It compensates. It routes the same organizational pattern through the segments that still move.
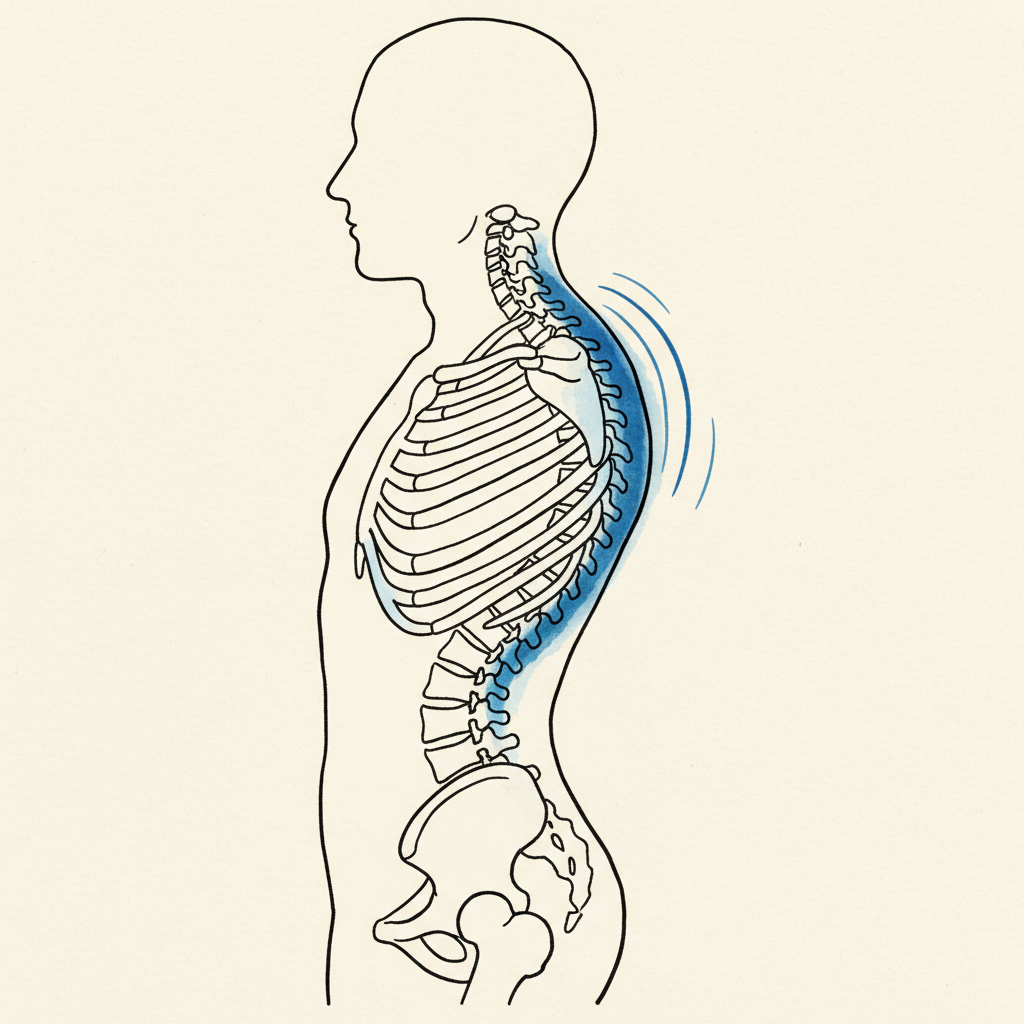
This leads to a well-documented phenomenon called adjacent segment disease. Helgeson’s 2010 review found that radiographic changes at segments adjacent to the fusion occur in a significant percentage of patients [4]. The fused segments are stable. The segments above and below bear new loads and receive the same neural instructions that generated the original curve.
Second, proximal junctional kyphosis. Hyun’s 2017 review documented this complication where the spine develops an acute kyphotic angle just above the top of the fusion construct [5]. The structural correction below creates a new mechanical demand above. The body schema adapts to the new hardware by reorganizing the unfused spine.
Neither of these complications is a failure of the surgery. They are the predictable consequence of correcting the output without updating the generator.
Think of it this way. The body schema is running a program. Fusion changes the hardware the program runs on. It does not change the program. The program routes through whatever hardware remains available.
Long-term complications after scoliosis spinal fusion include adjacent segment disease (ASD) and proximal junctional kyphosis (PJK). Helgeson’s 2010 systematic review documented radiographic adjacent segment changes in a significant percentage of fusion patients, occurring at segments immediately above and below the instrumented levels. Hyun’s 2017 review described PJK as an acute kyphotic deformity developing at the proximal junction of the fusion construct. These complications arise because fusion eliminates motion at the instrumented segments, transferring mechanical load to adjacent mobile segments. From a nervous system perspective, the body schema (Paillard 1999) continues generating the same organizational prediction through whatever segments remain mobile. The structural correction does not update the neural model that generated the curve. The prediction adapts to the new hardware.
What “failed conservative management” actually means
In most surgical consultations, there is a moment where the surgeon says something like: “We have tried conservative management and the curve has continued to progress.”
That statement is accurate within the conventional model. Physical therapy was attempted. Bracing was attempted. The curve progressed anyway. By the standards of the mechanical model, conservative options have been exhausted.
But what was actually assessed?
In most cases, “conservative management” means strengthening exercises targeting the muscles around the curve. Stretching the concavity. Bracing to mechanically constrain the curve. Observation to monitor progression. Physical therapy protocols that address the musculoskeletal system.
None of these assess the system generating the curve.
The SOSORT guidelines recommend exercise-based conservative treatment and establish evidence-based standards for non-surgical management [6]. This is important work. But the guidelines operate within a model that treats the curve as a structural and muscular problem. The body schema is not assessed. The prediction generating the curve is not assessed. The nervous system’s organizational strategy is not assessed.
“Failed conservative management” means the output was measured and the output did not change with the interventions applied. It does not mean the generative system was assessed and found incapable of producing a different output.
The standard is incomplete. Not wrong. Incomplete.
A curve that progressed through physical therapy and bracing has demonstrated that muscular and mechanical interventions were insufficient. It has not demonstrated that the nervous system prediction generating the curve cannot be updated. Because that prediction was never addressed.
This is the gap. Not a gap in surgical competence. A gap in the assessment model. The question “have we exhausted conservative options?” cannot be answered honestly if the generative system was never part of the conservative protocol.
In surgical consultations for scoliosis, “failed conservative management” typically means physical therapy, bracing, and observation did not prevent curve progression. The SOSORT 2018 guidelines (Negrini et al.) establish evidence-based standards for conservative scoliosis treatment including exercise-based approaches and bracing. However, conventional conservative management addresses the musculoskeletal system without assessing the nervous system prediction that generates the curve. The body schema (Paillard 1999) runs a continuous model that produces posture as output. If the prediction was never assessed or targeted, the statement “conservative management has failed” is incomplete. The curve progressed through interventions that addressed the output. The system generating the output was not part of the protocol. This does not mean surgery is wrong. It means the pre-surgical assessment may be incomplete.
Questions to ask your surgeon
These are not adversarial questions. They are informed questions. The kind a person asks when they want to understand the full scope of what they are deciding.
Does the surgical plan account for adjacent segment loading?
The Lenke classification determines which segments to fuse [1]. Ask specifically how the segments above and below the fusion are expected to respond. What monitoring will be in place for adjacent segment changes. What the plan is if proximal junctional kyphosis develops [5]. Good surgeons think about this. It is a reasonable question.
What is the revision rate for this specific procedure?
Not the general success rate. The revision rate. The percentage of patients who require a second surgery to address complications, hardware failure, or adjacent segment problems. This number is specific to the procedure being proposed, the curve type, and the surgeon’s volume. You deserve this number.
What conservative approaches were attempted, and what specifically did they address?
If the answer is “physical therapy and bracing,” ask a follow-up: did any of those approaches assess the nervous system’s organizational strategy? Did any of them target the body schema, the prediction model, the sensory inputs driving the curve? If the answer is no, that is not a reason to refuse surgery. It is a reason to understand that one category of conservative intervention has not been explored.
Has anyone assessed the system generating this curve? Not just measured the curve?
The Cobb angle measures the output. The body schema generates the output [3]. These are different things. A thorough pre-surgical workup should ideally account for both. If the generative system has not been assessed, you have information about the shape of the problem but not the source of the problem.
Ask these questions without antagonism. Write them down. Bring them to the consultation. A surgeon who takes them seriously is a surgeon who is thinking beyond the hardware.
What generative posture adds (whether you choose surgery or not)
The body schema model is not a replacement for surgery. It is a complement to whatever decision you make. Its value does not depend on choosing one path over the other. It applies to all three phases of the decision.
If you are still deciding.
Understanding the generative model gives you agency. Not the false agency of “you can fix this yourself if you try hard enough.” Real agency. The kind that comes from understanding what is actually happening in your body. From knowing what the curve is, what generates it, and what each intervention does and does not address.
Your posture is generated by a system. The curve is the output of that system [7]. Surgery changes the output at the fused segments. Generative posture work changes the system. Both are real interventions. They address different things. Your decision should account for both.
If you choose surgery.
Pre-operatively, generative posture work improves respiratory mechanics, autonomic regulation, and body awareness. These are not abstract benefits. Better respiratory function means better surgical recovery. Better autonomic regulation means the nervous system is not in a threat state going into anesthesia and tissue trauma. Better body awareness means more accurate rehabilitation.
Post-operatively, the work shifts to sensory re-education of the unfused segments. Respiratory rehabilitation. Nervous system regulation during the recovery period. And adaptation to the new biomechanics. The body schema needs to update its model to account for the structural changes surgery created. Without that update, the schema continues running its old prediction through the segments that still move.
This is where adjacent segment problems originate. Not from surgical failure. From the body schema continuing to generate its pre-surgical prediction through post-surgical anatomy. Generative posture work after surgery is the bridge between the structural correction and the neural update.
If you choose not to have surgery.
Then the generative model becomes the primary intervention. The body schema is addressed directly. The prediction is updated through novel sensory input that the system cannot dismiss [7]. The complete guide to non-surgical scoliosis treatment maps this territory in detail.
The point is this: generative posture work is not positioned against surgery. It is positioned alongside the entire decision. Before. During recovery. After. Or instead. The value holds regardless of the surgical decision because the body schema is always running.
Preparation before scoliosis surgery can improve outcomes, but the type of preparation matters. Standard pre-surgical physical therapy addresses muscle conditioning and flexibility. Generative posture preparation addresses the nervous system prediction that organizes the spine. Research on the body schema (Paillard 1999) and predictive coding (Friston 2010) shows that posture is generated by an internal neural model. Spinal fusion changes the structural output but does not update this model. Post-operatively, the body schema continues generating its pre-surgical prediction through unfused segments, contributing to adjacent segment disease (Helgeson 2010) and proximal junctional kyphosis (Hyun 2017). Pre-surgical nervous system preparation (respiratory mechanics, autonomic regulation, body awareness) and post-surgical sensory re-education may help the body schema update its model to account for the new biomechanical reality. This is complementary to surgery, not a replacement for it.
Before scoliosis surgery, asking informed questions improves decision quality. Key questions include: Does the surgical plan account for adjacent segment loading, given that Helgeson’s 2010 review documented radiographic changes at segments adjacent to the fusion? What is the revision rate for this specific procedure and curve type? What conservative approaches were attempted and what specifically did they target (musculoskeletal system only, or also the nervous system prediction generating the curve)? The SOSORT 2018 guidelines (Negrini et al.) recommend exercise-based conservative treatment, but standard protocols do not assess the body schema (Paillard 1999), the brain’s internal model that generates posture as a prediction (Friston 2010). “Failed conservative management” in most surgical contexts means physical therapy and bracing did not arrest progression. It does not necessarily mean the generative system was assessed and found unable to produce a different output. These questions are not adversarial. They are the questions a fully informed patient asks.
The position
We are not telling you what to decide.
We are telling you what to assess before you decide.
The conventional surgical pathway measures the curve, tracks the progression, applies conservative interventions aimed at the musculoskeletal system, and recommends surgery when those interventions do not arrest progression. That pathway is medically sound. It follows the evidence within its model.
But the model is incomplete. The system that generates the curve is not assessed. The body schema is not part of the conservative protocol. The prediction is not addressed. And when conservative management is declared to have failed, it has failed at the muscular level. It has not been attempted at the generative level.
A fully informed decision accounts for both. The structural reality of the curve. And the generative system producing it.
If you are weighing surgery, you deserve to know what surgery does well, what it does not address, what questions to ask, and what options exist for the part of the problem surgery was not designed to solve. This article is that information.
If you want to understand the history of the mechanical model that most surgical decisions are made within, that context matters. If you want to understand what non-surgical treatment looks like when it targets the generative system, that map exists.
The decision is yours. We want it to be a complete one.
—
About the author: Sam Miller is the creator of Syntropic Core and founder of Posture Dojo. Diagnosed with an 85-degree kyphoscoliosis at 13, he spent two decades mapping the nervous system mechanisms that conventional treatment misses. He works with people whose bodies did not respond to the standard playbook. His approach is built on the predictive neuroscience of posture, not the mechanical model that failed him.
Ready to go deeper? Learn about Syntropic Core Reset and discover what treatment looks like when it targets the prediction, not just the curve.
Syntropic Core Reset
Most posture programs give you exercises. This one updates the system that generates your posture. Four weeks live with Sam Miller. You learn how the hidden map works, why everything else missed it, and how to give your nervous system the evidence it needs to generate a different pattern. Breath. Ground contact. Safety. Sensory input. Floor to standing. You leave with a daily practice that holds because the map itself has changed.
Limited spots. Next cohort enrolling now.
Sources
- Lenke, L.G., Betz, R.R., Harms, J., Bridwell, K.H., Clements, D.H., Lowe, T.G., & Blanke, K. (2001). Adolescent idiopathic scoliosis: a new classification to determine extent of spinal arthrodesis. Journal of Bone and Joint Surgery, 83-A(8), 1169-1181. [T1]
The Lenke classification system for surgical planning. Six curve types determining which segments to fuse. Standard of care for operative decision-making.
- Weinstein, S.L., Dolan, L.A., Wright, J.G., & Dobbs, M.B. (2013). Effects of bracing in adolescents with idiopathic scoliosis. New England Journal of Medicine, 369(16), 1512-1521. [T1]
BrAIST study confirming bracing reduces curve progression in AIS. Establishes that curves above surgical threshold progress without intervention.
- Paillard, J. (1999). Body schema and body image: a double dissociation in deafferented patients. In G.N. Gantchev, S. Mori, & J. Massion (Eds.), Motor Control, Today and Tomorrow (pp. 197-214). Sofia: Academic Publishing House. [T1]
Body schema as the non-conscious sensorimotor model generating posture. The distinction between the predictive model (schema) and the perceived image.
- Helgeson, M.D., Shah, S.A., Newton, P.O., Clements, D.H., Betz, R.R., Marks, M.C., & Bastrom, T. (2010). Evaluation of proximal junctional kyphosis in adolescent idiopathic scoliosis following pedicle screw, hook, or hybrid instrumentation. Spine, 35(2), 177-181. [T1]
Adjacent segment disease after scoliosis fusion. Radiographic changes at segments adjacent to fusion construct documented in significant percentage of patients.
- Hyun, S.J., Lee, J., & Lee, B.H. (2017). Proximal junctional kyphosis and proximal junctional failure following adult spinal deformity surgery. Korean Journal of Spine, 14(4), 126-132. [T1]
PJK as a documented complication after spinal deformity surgery. Acute kyphotic angle development above fusion construct.
- Negrini, S., Donzelli, S., Aulisa, A.G., et al. (2018). 2016 SOSORT guidelines: orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis and Spinal Disorders, 13, 3. [T1]
Evidence-based conservative treatment guidelines. Exercise-based approaches recommended. Does not include body schema assessment in conservative protocol.
- Friston, K. (2010). The free-energy principle: a unified brain theory? Nature Reviews Neuroscience, 11(2), 127-138. [T1]
Predictive coding framework. The brain generates posture as a prediction. Scoliosis as a prediction the nervous system maintains, not a structural defect.