The eye is a postural organ
Most people understand vision as the sense that lets them see. The eye is doing two things at once, and only one of them is for seeing.
The other thing the eye is doing is feeding the postural system the single largest stream of spatial information about where your body is in space. Your nervous system uses the visual horizon to set head position. It uses ocular convergence to map distance. It uses the difference between the two retinal images to construct depth. It uses peripheral motion to set tone in the trunk and legs.
When any of this is asymmetric, the body has a choice. It can let the eyes see a tilted, unstable, or asymmetric world. Or it can tilt and rotate the body to compensate. The body almost always chooses to tilt and rotate.
That tilt is posture. Often it is also scoliosis.
This article explains why vision sits at the top of the postural hierarchy, what happens when it goes wrong, and what to do when a structural practitioner finally tells you the eyes are part of the case.
The 158-word answer
Vision sits at the top of the postural hierarchy. The brain prioritizes a level visual horizon, stable binocular convergence, and ambient peripheral input above almost every other sensory channel. When any of these is asymmetric or compromised, the body generates a compensating posture (head tilt, shoulder rotation, pelvic shift) to restore visual stability. This is the predictive postural system doing exactly what it is built to do. Behavioral optometrists, a specialty inside developmental vision care, screen for the visual asymmetries that drive postural compensation. Ambient vision (the unconscious peripheral channel that feeds posture) is distinct from focal vision (the central channel used for reading). Most eye exams test only the focal channel and miss the ambient. When the ambient channel is dysfunctional, no amount of spinal therapy will hold against it. Vision therapy, prism lenses, and syntonic light therapy address the upstream problem. For adults with scoliosis, kyphosis, or chronic forward head, vision screening is often the missing variable.
Two visual systems, only one of which most exams test
Behavioral optometrists distinguish two functionally different visual streams [1].
Focal vision is the central, high-resolution channel. It is what you use to read, recognize faces, and identify objects. This is the channel that gets tested at a routine eye exam. Can you read this line, can you read that line, are your prescriptions correct. Focal vision is what we usually mean when we say we can see.
Ambient vision is the peripheral, low-resolution channel. It is what you use to know where the floor is without looking, where the doorframe is in your peripheral field, whether the world is tilted, whether something is moving toward you in the side of your visual field. Ambient vision runs largely unconsciously. It feeds directly into the postural system through the superior colliculus, the vestibular nuclei, and the cerebellum.
Ambient vision is the postural channel.
A routine eye exam tests focal vision. It barely touches the ambient channel. You can have twenty-twenty focal acuity and a severely compromised ambient system, walk out of the exam with a clean bill of visual health, and never connect your chronic forward head, your shoulder asymmetry, or your stalled scoliosis progress to your eyes.
The behavioral optometrist tests both.
Why an asymmetric visual system produces an asymmetric body
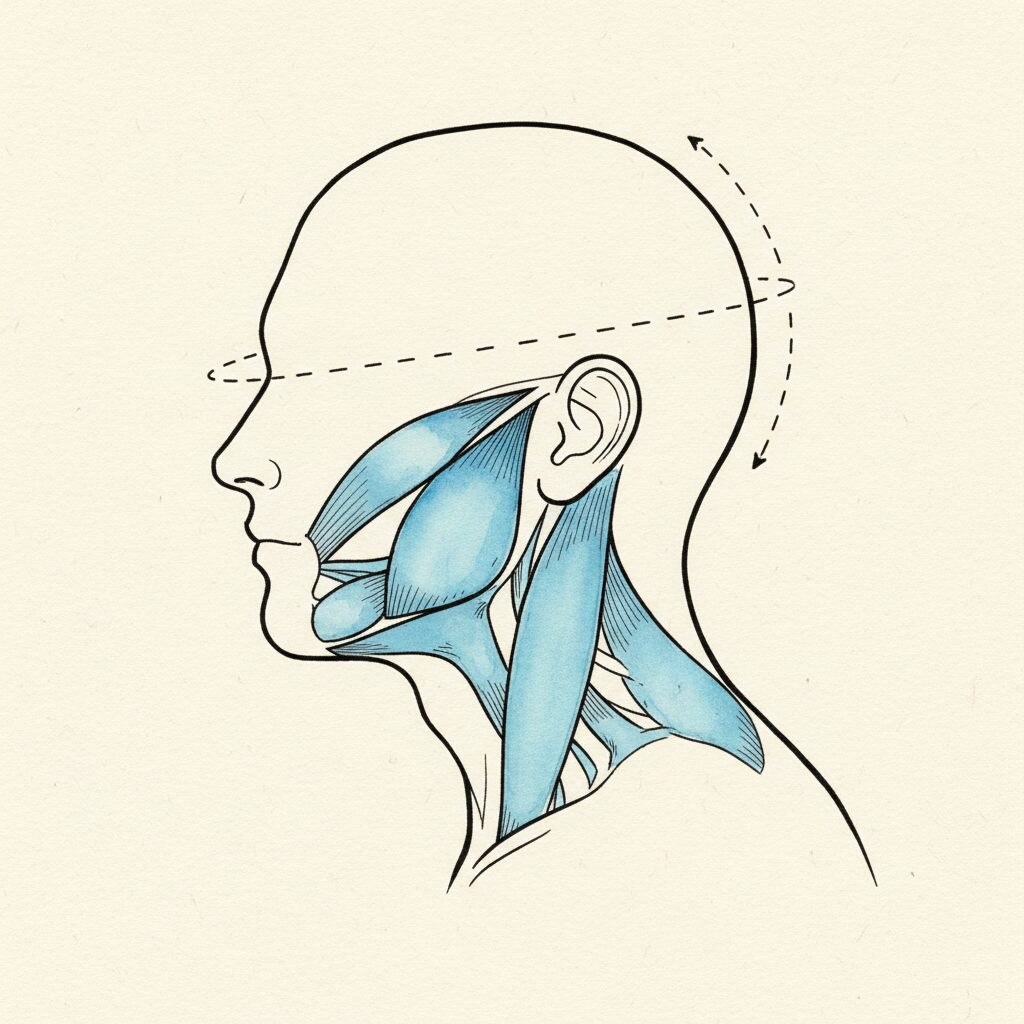
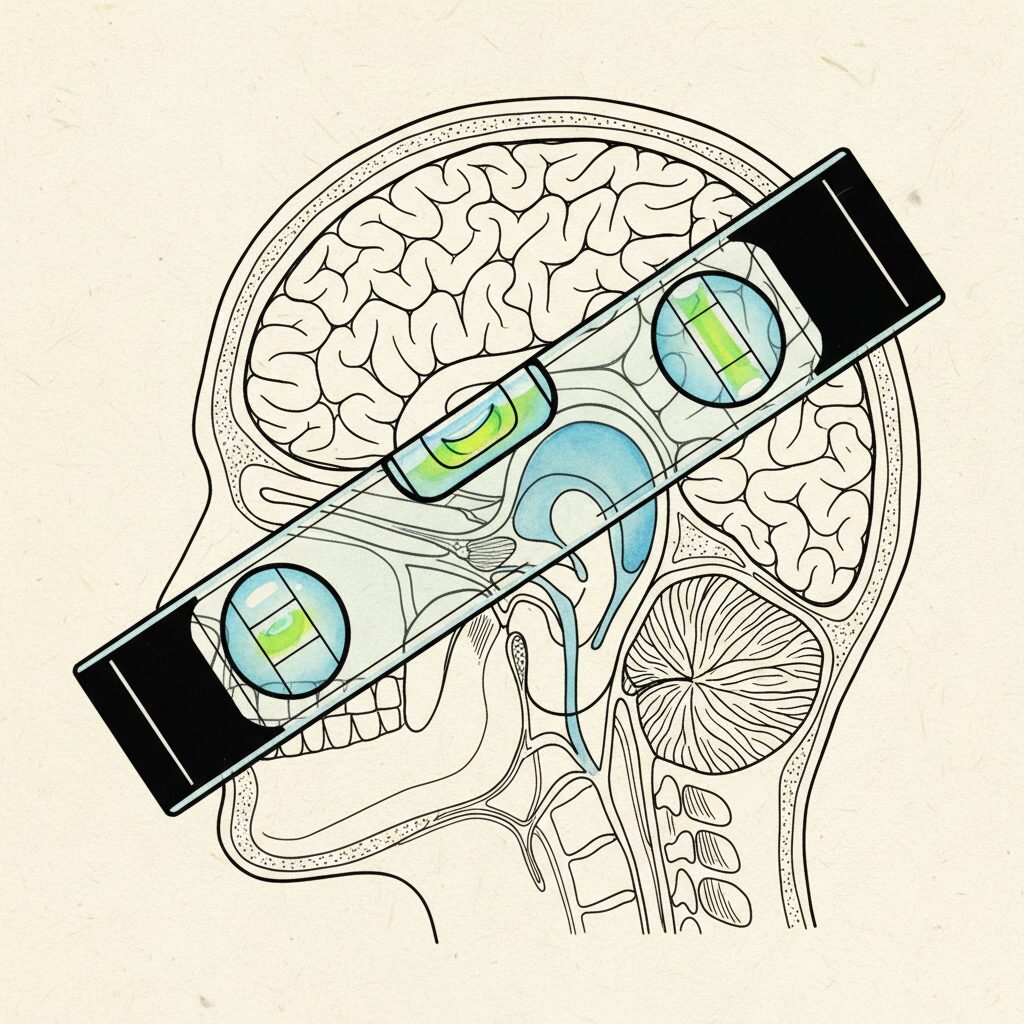
Your nervous system holds a few things sacred. The visual horizon being level is one of them. The brain treats a tilted horizon the way it treats a fire alarm. It will reorganize everything downstream to make the alarm stop.
If your eyes do not converge symmetrically, if one eye is dominant in a way that pulls visual attention sideways, if your ambient field is constricted on one side, the brain receives a tilted or asymmetric world. It compensates by tilting the head to level the horizon. The neck adapts. The shoulders rotate. The thoracic spine adapts. The pelvis shifts to keep the head over the base of support [3].
Within months, the body has reorganized into a curved or rotated shape that, from outside, looks like a postural problem. From inside, it is the body solving an information problem the only way it knows how.
This is the same logic that produces curves in response to vestibular asymmetry. The eye and the vestibular system are tightly coupled. Both feed the spatial-orientation networks in the brainstem and cerebellum. Both have to agree on where level is. When they disagree, the body picks one and bends to it.
Where vision dysfunction shows up in your body
The signs that the visual system may be driving your postural pattern are not subtle once you know what to look for.
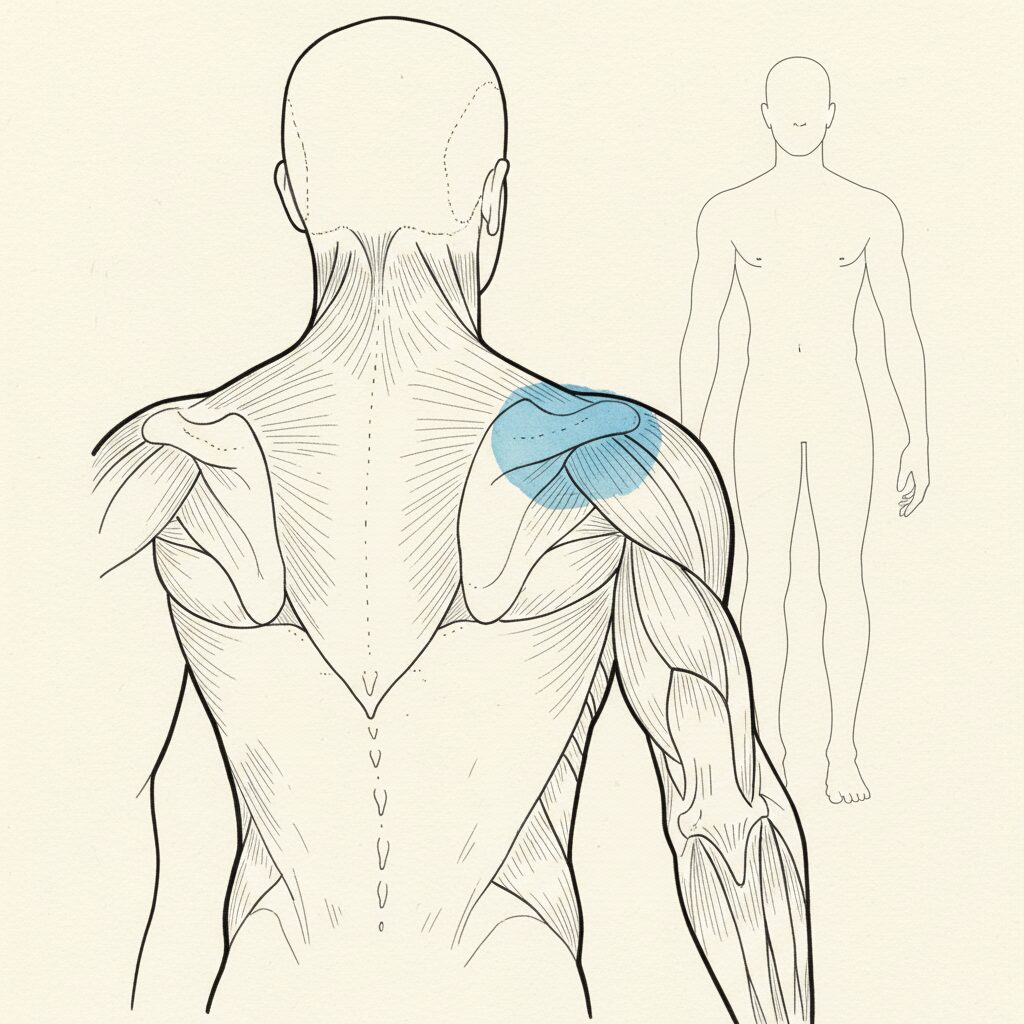
Forward head posture that does not respond to neck-specific work. The head is forward because that is where the visual system is finding the most stable image. Strengthening the neck does not address the visual driver.
Shoulder asymmetry that mirrors eye dominance. If you are right-eye dominant and right-shoulder elevated, the body is pulling toward the dominant eye. If the dominance is severe, the curve goes with it.
Reading-induced neck and back fatigue. The eyes are working harder than they should to coordinate convergence. The body braces to assist. Hours into a screen day, the neck and upper back are paying the visual bill.
Carsickness or screen-induced nausea that started in adulthood. The ambient-versus-focal channels are out of sync. The vestibular system disagrees with the visual system. Posture is downstream of both.
Chronic mild head tilt that you have been told to correct. The tilt is solving a visual problem. Cueing it away without addressing the visual problem does not change the underlying asymmetry. It just adds tension on top of it.
Scoliosis or kyphosis that responded partially to physical therapy and then plateaued. The plateau is often where the visual driver becomes the rate limiter. Until vision moves, the structure cannot.
The behavioral optometry workup
A behavioral optometry exam is not the same as a routine eye exam. The intake includes binocular vision testing under load, ambient-field screening, ocular dominance and tracking assessment, postural responses to prism and tinted lenses, and integration testing across vision, vestibular, and proprioceptive channels [1].
The interventions that come out of this workup include vision therapy (a structured set of exercises that retrain convergence, accommodation, and ambient-focal integration), prism lenses (which shift the visual field to give the body a level horizon before the body has to compensate), and in some clinics syntonic light therapy (which uses specific wavelengths to address visual-field constriction).
The treatment timeline varies. Some adults experience postural change within weeks of starting prism. Others run a vision therapy protocol for three to nine months before the postural system fully reorganizes. The point is that the upstream change is what makes the downstream change possible. Without it, the spinal work is rowing against current.
When PSSE alone is not enough
The PSSE family of scoliosis methods (Schroth, BSPTS-Rigo, SEAS) is excellent for what it is built to do. It loads the spine in three-dimensional correction patterns, teaches rotational breathing, and produces measurable changes in Cobb angle in many patients.
What PSSE does not do, in its standard form, is address the visual or vestibular drivers feeding into the postural prediction loop. Some clinicians integrate visual screening into their PSSE protocols. Most do not.
If a patient runs a clean PSSE protocol (Schroth, BSPTS-Rigo, SEAS) for six to twelve months and the curve does not move, the question to ask is whether an upstream input is overriding the corrective work. Vision and vestibular function are the most common candidates.
The structural therapy is not failing. It is being asked to overpower an upstream signal that nobody on the team is addressing.
The strongest scoliosis outcomes in adult care tend to come from a small team. A PSSE-trained physical therapist, a behavioral optometrist, a myofunctional therapist or jaw-trained dentist, and someone reading nervous system state across all of it. Each one is treating a different layer of the same case.
What to ask a behavioral optometrist
A few questions to bring to the first visit.
Do you screen ambient versus focal vision separately. The answer should be yes. If it is no, you are looking at a routine eye exam in a different building.
Do you test ocular dominance and binocular convergence under postural load. Strong answer: yes, we test how the visual system responds when the body is asked to move, not just when it is still.
Do you work with prism, tinted lenses, or syntonic light therapy. Some practitioners use one tool. Others use all three. The tools should be matched to the case, not the case to the tools.
How do you coordinate with other practitioners on a scoliosis case. The strong behavioral optometrist will name physical therapists, myofunctional therapists, and craniofacial dentists they routinely partner with. The weak one treats vision as a standalone problem.
Find a behavioral optometrist
The CSCN practitioner directory tags every practitioner by upstream specialty. Filter the directory by Visual System to surface behavioral optometrists, developmental optometrists, and neuro-visual rehabilitation practitioners in your region.
Browse the directory filtered by Visual System. If you are running a PSSE protocol that has plateaued, this is often the missing variable. Pair vision care with a Schroth or PSSE practitioner and a jaw-screening clinician for the strongest adult-scoliosis outcomes.
FAQ
Can vision problems cause scoliosis?
Visual asymmetry is not the sole cause of scoliosis in most cases. It is, however, one of the upstream inputs that can drive postural asymmetry and accelerate or maintain a curve. Treating the visual contributor often unsticks cases that have plateaued on structural therapy alone [1].
What is behavioral optometry?
Behavioral optometry is a sub-specialty inside optometry that addresses the relationship between vision, posture, balance, and learning. Behavioral optometrists test the visual system functionally (how it integrates with movement, attention, and posture) rather than testing only acuity. They are also called developmental optometrists or neuro-rehabilitation optometrists.
Will prism glasses fix my posture?
Prism lenses can produce measurable postural change in patients whose body is compensating for visual asymmetry. They are not a cure for established structural changes. They remove the visual driver so the postural system can reorganize. The structural work still has to happen, but it works better when the upstream signal stops fighting it.
How is a behavioral optometry exam different from a regular eye exam?
A regular eye exam tests focal acuity and corrects refractive errors. A behavioral optometry exam tests both ambient and focal channels, binocular vision under load, ocular tracking, dominance, postural responses to lenses, and integration with vestibular and proprioceptive function. The exam takes longer and produces a treatment plan that often includes vision therapy.
Is vision therapy worth it for adults with scoliosis or chronic posture problems?
For cases where structural therapy has plateaued, where there is significant head tilt, or where reading and screen work produce disproportionate neck and back fatigue, vision therapy is often the highest-leverage intervention available. Outcomes vary by case. The screening exam, even on its own, often clarifies whether vision is part of the picture.
Sources
- Padula WV, Munitz R, Magrun WM. Neuro-Visual Processing Rehabilitation: An Interdisciplinary Approach. Optometric Extension Program Foundation. 2012.
- Padula WV, Argyris S, Ray J. Visual evoked potentials (VEP) evaluating treatment for post-trauma vision syndrome (PTVS) in patients with traumatic brain injuries (TBI). Brain Inj. 1994;8(2):125-133. PMID 8193551.
- Gagey PM, Weber B. Posturologie: Régulation et dérèglements de la station debout. 3rd ed. Masson. 2008.
- Matheron E, Yang Q, Lê TT, Kapoula Z. Effects of ocular dominance on the vergence eye movements. PLoS One. 2008;3(11):e3777. PMID 19015735.
- Kapoula Z, Lê TT. Effects of distance and gaze position on postural stability in young and old subjects. Exp Brain Res. 2006;173(3):438-445. PMID 16525804.